

Missing and unerupted teeth in osteogenesis imperfecta
- PMID: 34020077
- PMCID: PMC12211518
- DOI: 10.1016/j.bone.2021.116011
Missing and unerupted teeth in osteogenesis imperfecta
Abstract
Introduction: Osteogenesis imperfecta (OI) is a genetic disorder characterized by bone fragility and craniofacial and dental abnormalities such as congenitally missing teeth and teeth that failed to erupt which are believed to be doubled in OI patients than normal populations and were associated with low oral health quality of life. However, the etiology of these abnormalities remains unclear. To understand the factors influencing missing and unerupted teeth, we investigated their prevalence in a cohort of OI patients as a function of the clinical phenotype (OI type), the genetic variant type, the tooth type and the onset of bisphosphonate treatment.
Method: A total of 144 OI patients were recruited from The Shriners Hospital, Montreal, Canada, between 2016 and 2017. Patients were evaluated using intraoral photographs and panoramic radiographs. Missing teeth were evaluated in all patients, and unerupted teeth were assessed only in patients ≥15 years old (n = 82).
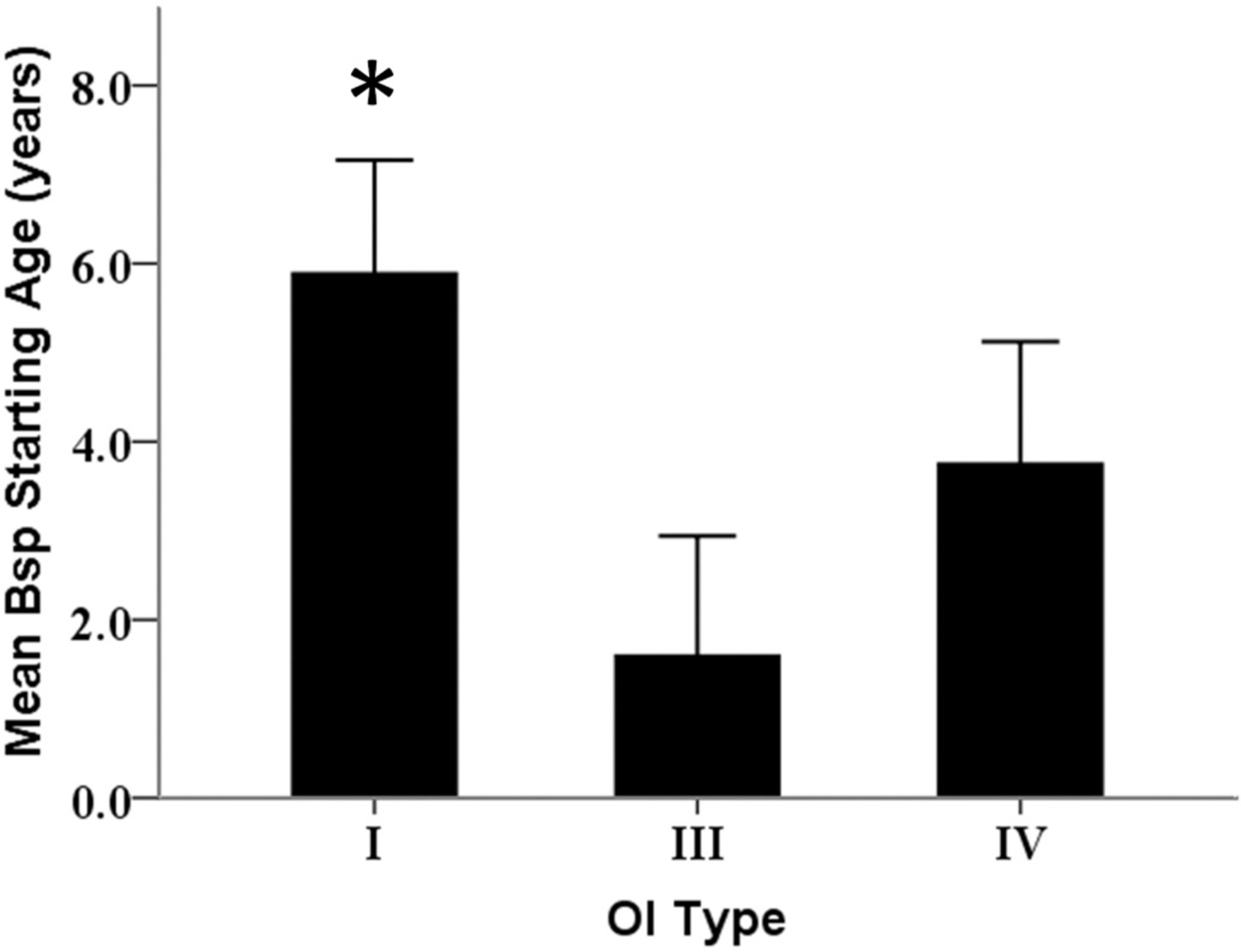
Results: On average, each OI patient had 2.4 missing teeth and 0.8 unerupted teeth, and the most common missing and unerupted teeth were the premolars and the upper second molars, respectively. These phenomena were more prominent in OI type III and IV than in OI type I, and were not sex or age-related. Missing teeth were significantly more common in patients with C-propeptide variants than all other variants (p-value <0.05). Unerupted teeth were significantly more common in patients with α1 and α2 glycine variants or substitutions than in those with haploinsufficiency variants. Early-onset of bisphosphonate treatment would significantly increase the risk of unerupted teeth in patients with OI types III and IV (OR = 1.68, 95% CI (1.15-1.53)).
Conclusion: The prevalence of missing and unerupted teeth at the tooth type level in OI patients varies according to the nature of the collagen variants and the OI type. These findings highlight the role of collagen in tooth development and eruption.
Keywords: Agenesis; Bisphosphonate; Missing teeth; Osteogenesis imperfecta; Rare disease; Retained teeth; Tooth development; Tooth eruption; Unerupted.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest
Authors declare no conflicts of interest.
Figures




References
-
- Glorieux FH, Osteogenesis imperfecta, Best Pract. Res. Clin. Rheumatol 22 (1) (2008) 85–100. - PubMed
-
- Stoll C, Dott B, Roth M-P, Alembik Y, Birth prevalence rates of skeletal dysplasias, Clin. Genet 35 (2) (1989) 88–92. - PubMed
-
- Andersen PE Jr., Hauge M, Osteogenesis imperfecta: a genetic, radiological, and epidemiological study, Clin. Genet 36 (4) (1989) 250–255. - PubMed
-
- Sillence DO, Rimoin DL, Classification of osteogenesis imperfect, Lancet. 1 (8072) (1978) 1041–1042. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
