

A progressive-individualized midstance gait perturbation protocol for reactive balance assessment in stroke survivors
- PMID: 34020123
- PMCID: PMC8228467
- DOI: 10.1016/j.jbiomech.2021.110477
A progressive-individualized midstance gait perturbation protocol for reactive balance assessment in stroke survivors
Abstract
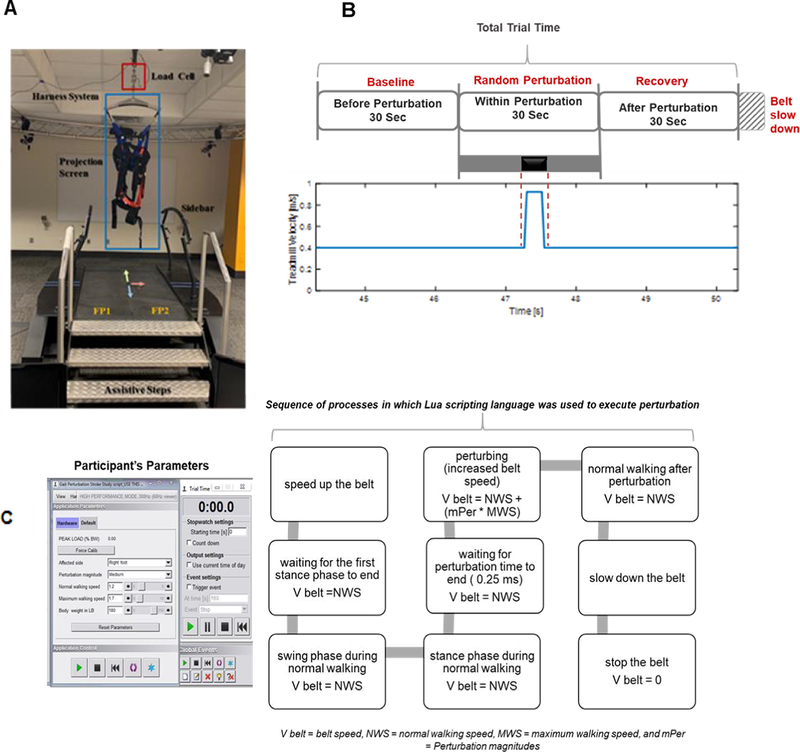
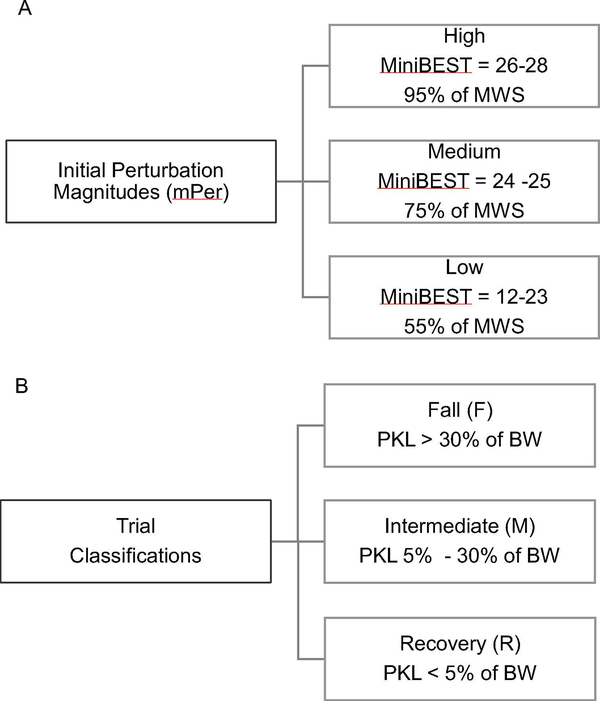
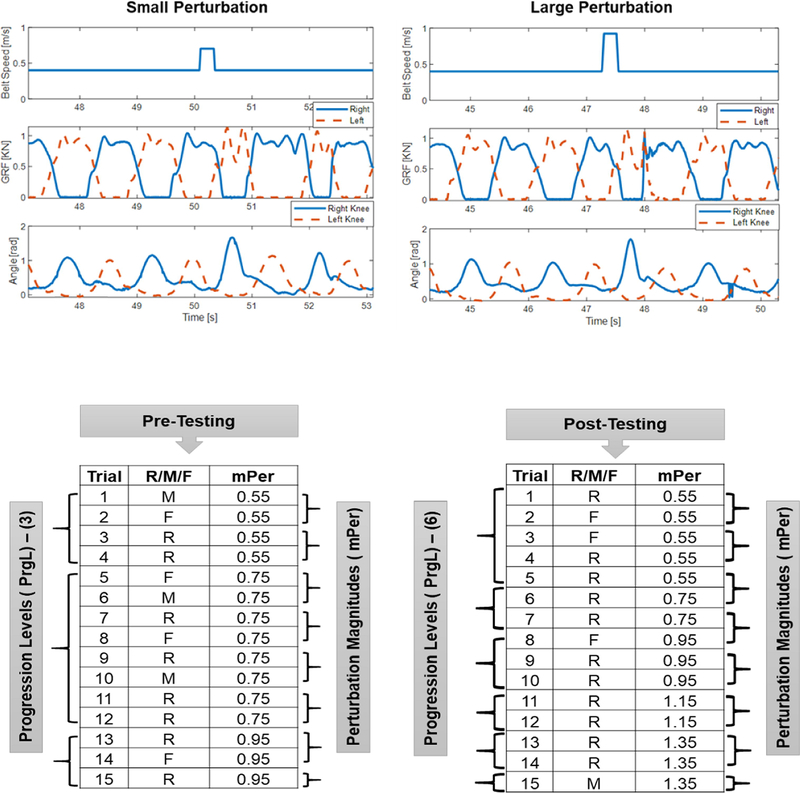
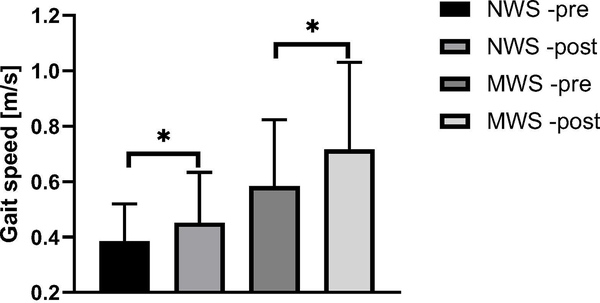
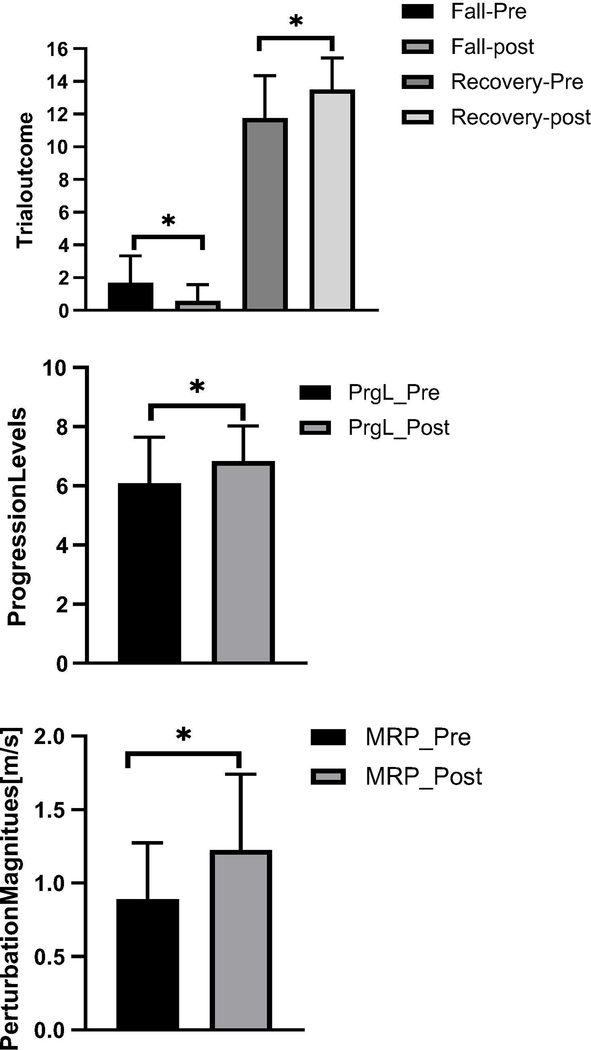
Restoration of balance control is a primary focus of rehabilitation after a stroke. The study developed a gait perturbation, treadmill-based, balance assessment protocol and demonstrated that it can be used to quantify improvements in reactive balance responses among individuals post-stroke. The protocol consists of a sequence of fifteen 90-second treadmill walking trials, with a single perturbation applied during the middle third of each trial. Gait was perturbed by rapid acceleration-deceleration of the treadmill belt at mid-stance of the unaffected leg during a randomly selected gait cycle. The initial perturbation magnitude was based on the participant's maximum walking speed and increased or decreased in each trial, based on success or failure of recovery, as determined from an instrumented harness. The protocol was used before and after a 10-week period of therapy in twenty-four stroke survivors. Outcomes included maximum recoverable perturbation (MRP), self-selected gait speed, levels progressed through the algorithm, and falls versus recoveries.Participants were able to take recovery steps in response to the perturbation. Twelve participants completed the full assessment protocol before and after the therapeutic intervention. After the intervention, they had fewer falls and more recoveries (p < 0.001), progressed through more algorithm levels (p = 0.043), had a higher MRP (p = 0.005), and had higher gait speeds. The protocol was found to be feasible in stroke survivors with moderate gait deficits. The data supports the conclusion that this protocol can be used in clinical research to quantify improvements in balance during walking.
Keywords: Falls; Gait; Mid-stance perturbation; Reactive balance; Stroke survivors.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest
Authors declare no conflicts of interest.
Figures
Similar articles
-
Feasibility of robot-based perturbed-balance training during treadmill walking in a high-functioning chronic stroke subject: a case-control study.J Neuroeng Rehabil. 2018 Apr 11;15(1):32. doi: 10.1186/s12984-018-0373-z. J Neuroeng Rehabil. 2018. PMID: 29642921 Free PMC article.
-
Transfer of reactive balance adaptation from stance-slip perturbation to stance-trip perturbation in chronic stroke survivors.Restor Neurol Neurosci. 2019;37(5):469-482. doi: 10.3233/RNN-190924. Restor Neurol Neurosci. 2019. PMID: 31561399
-
More symmetrical gait after split-belt treadmill walking does not modify dynamic and postural balance in individuals post-stroke.J Electromyogr Kinesiol. 2018 Aug;41:41-49. doi: 10.1016/j.jelekin.2018.04.008. Epub 2018 Apr 24. J Electromyogr Kinesiol. 2018. PMID: 29747067
-
[Reactive dynamic balance in the geriatric setting : Possibilities for evaluation and quantification in functionally heterogeneous persons].Z Gerontol Geriatr. 2023 Oct;56(6):458-463. doi: 10.1007/s00391-023-02227-7. Epub 2023 Sep 1. Z Gerontol Geriatr. 2023. PMID: 37656226 Review. German.
-
A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults.Eur Rev Aging Phys Act. 2017 Mar 2;14:3. doi: 10.1186/s11556-017-0173-7. eCollection 2017. Eur Rev Aging Phys Act. 2017. PMID: 28270866 Free PMC article. Review.
Cited by
-
Physical rehabilitation approaches for the recovery of function and mobility following stroke.Cochrane Database Syst Rev. 2025 Feb 11;2(2):CD001920. doi: 10.1002/14651858.CD001920.pub4. Cochrane Database Syst Rev. 2025. PMID: 39932103 Free PMC article.
References
-
- Daly JJ et al. (2011) ‘Recovery of coordinated gait: Randomized controlled stroke trial of functional electrical stimulation (FES) versus no FES, with weight-supported treadmill and over-ground training’, Neurorehabilitation and Neural Repair, 25(7), pp. 588–596. doi: 10.1177/1545968311400092. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
