

Peritoneal or mesenteric tumours revealing histiocytosis
- PMID: 34020934
- PMCID: PMC8144026
- DOI: 10.1136/bmjgast-2021-000622
Peritoneal or mesenteric tumours revealing histiocytosis
Abstract
Objective: Peritoneal or mesenteric tumours may correspond to several tumour types or tumour-like conditions, some of them being represented by histiocytosis. This rare condition often poses diagnostic difficulties that can lead to important time delay in targeted therapies. Our aim was to describe main features of histiocytoses with mesenteric localisation that can improve the diagnostic process.
Design: We performed a retrospective study on 22 patients, whose peritoneal/mesenteric biopsies were infiltrated by histiocytes.
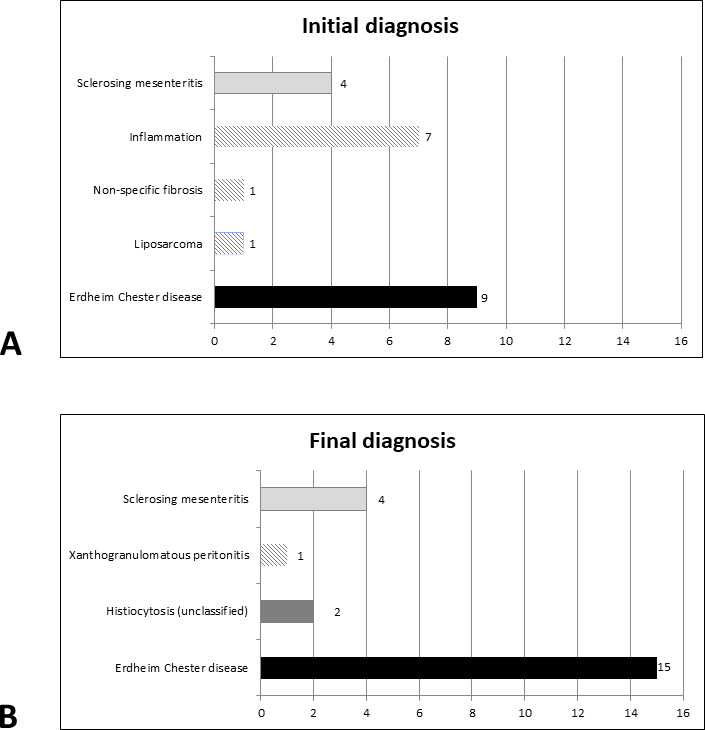
Results: Abdominal pain was the revealing symptom in 10 cases, and 19 patients underwent surgical biopsies. The diagnosis of histiocytosis was proposed by initial pathologists in 41% of patients. The other initial diagnoses were inflammation (n=7), sclerosing mesenteritis (n=4) and liposarcoma (n=1). The CD163/CD68+CD1a- histiocytes infiltrated subserosa and/or deeper adipose tissues in 16 and 14 cases, respectively. A BRAFV600E mutation was detected within the biopsies in 11 cases, and two others were MAP2K1 mutated. The final diagnosis was histiocytosis in 18 patients, 15 of whom had Erdheim-Chester disease. The median diagnostic delay of histiocytosis was 9 months. Patients treated with BRAF or MEK inhibitors showed a partial response or a stable disease. One patient died soon after surgery, and five died by the progression of the disease.
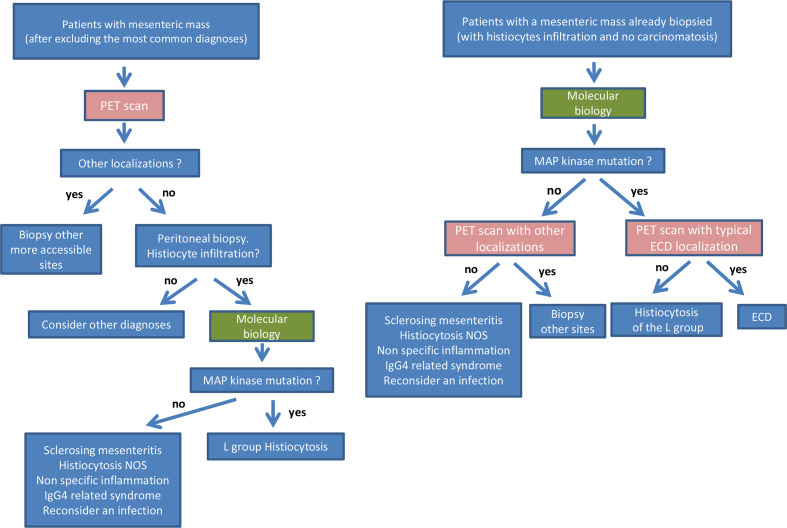
Conclusion: Diagnosis of masses arising in the mesentery should be carefully explored as one of the possibilities in histiocytosis. This diagnosis is frequently missed on mesenteric biopsies. Molecular biology for detecting the mutations in BRAF or in genes of the MAP kinase pathway is a critical diagnostic tool.
Keywords: abdominal pain; cancer; molecular biology.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous