

Metabolomics Profiling of Patients With A-β+ Ketosis-Prone Diabetes During Diabetic Ketoacidosis
- PMID: 34021044
- PMCID: PMC8385613
- DOI: 10.2337/db21-0066
Metabolomics Profiling of Patients With A-β+ Ketosis-Prone Diabetes During Diabetic Ketoacidosis
Abstract
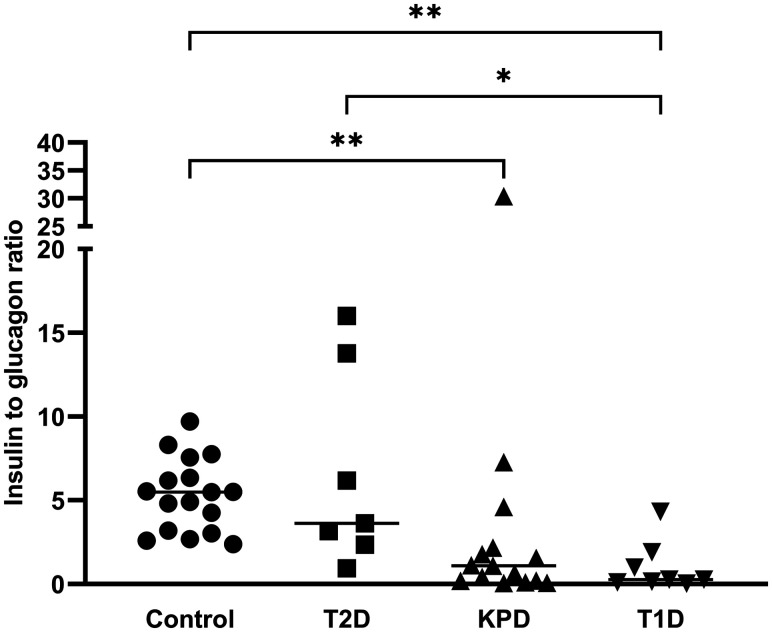
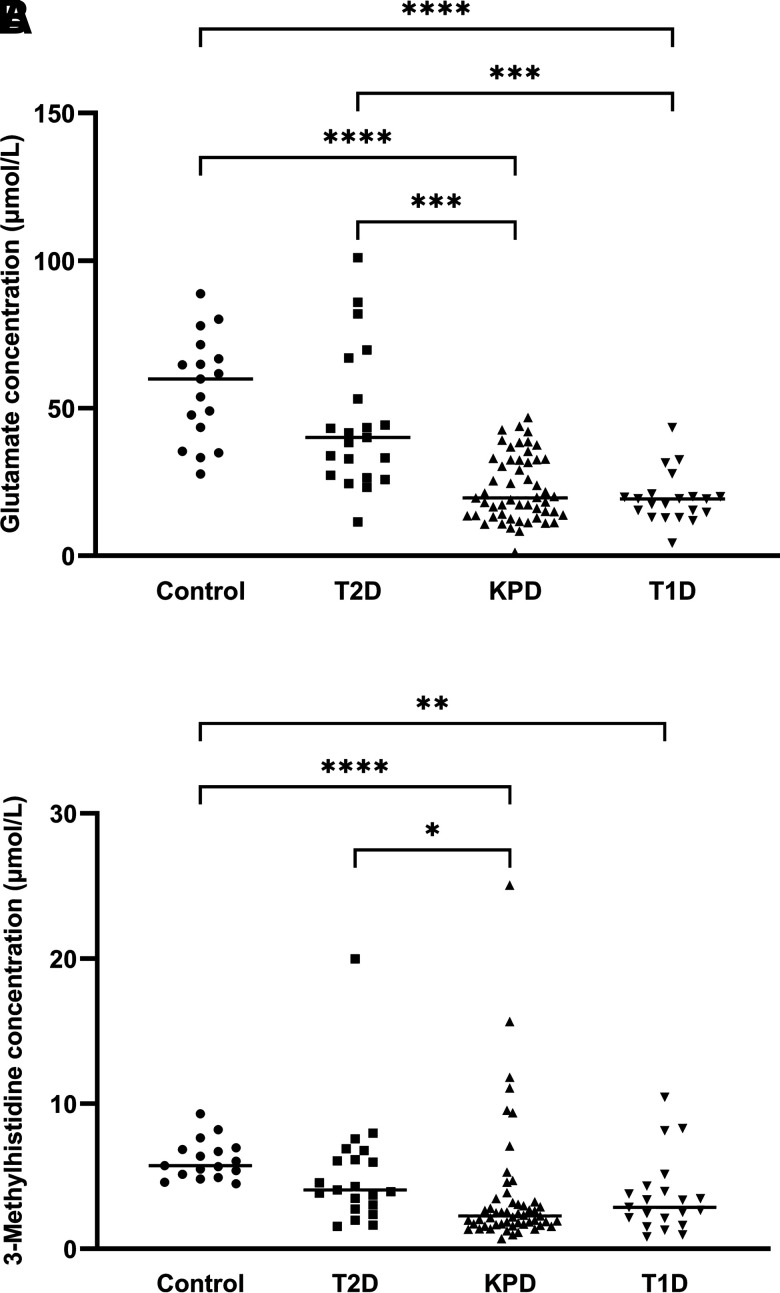
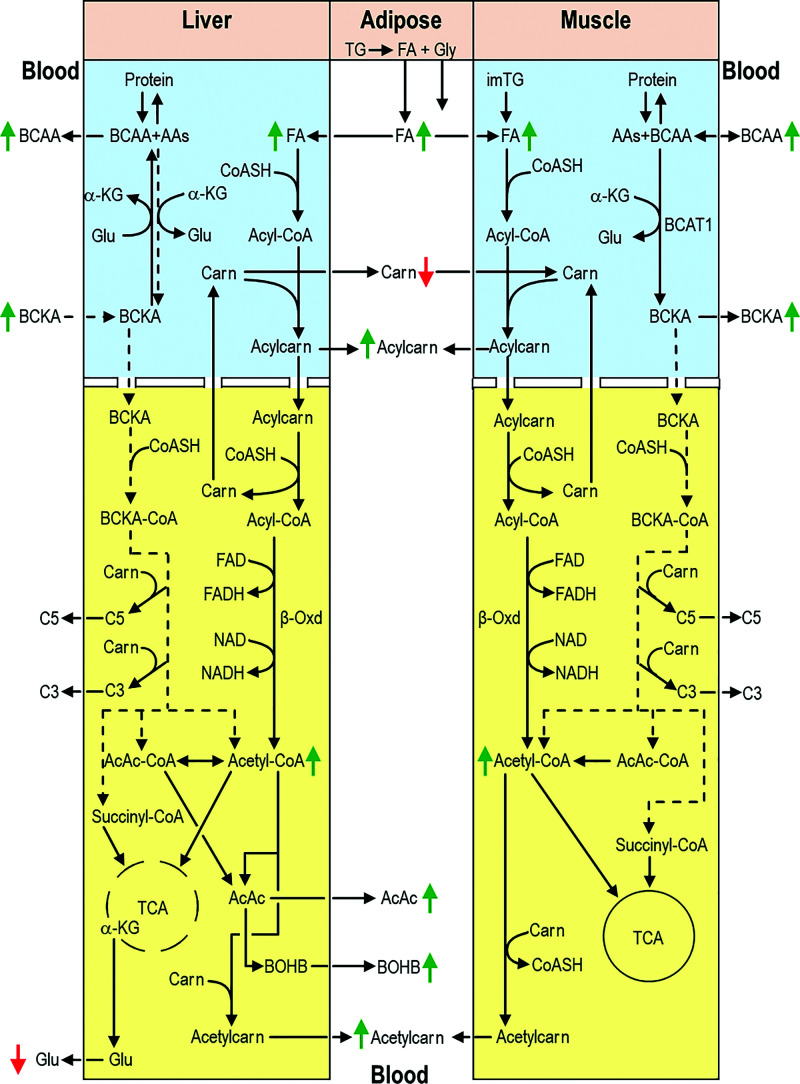
When stable and near-normoglycemic, patients with "A-β+" ketosis-prone diabetes (KPD) manifest accelerated leucine catabolism and blunted ketone oxidation, which may underlie their proclivity to develop diabetic ketoacidosis (DKA). To understand metabolic derangements in A-β+ KPD patients during DKA, we compared serum metabolomics profiles of adults during acute hyperglycemic crises, without (n = 21) or with (n = 74) DKA, and healthy control subjects (n = 17). Based on 65 kDa GAD islet autoantibody status, C-peptide, and clinical features, 53 DKA patients were categorized as having KPD and 21 type 1 diabetes (T1D); 21 nonketotic patients were categorized as having type 2 diabetes (T2D). Patients with KPD and patients with T1D had higher counterregulatory hormones and lower insulin-to-glucagon ratio than patients with T2D and control subjects. Compared with patients withT2D and control subjects, patients with KPD and patients with T1D had lower free carnitine and higher long-chain acylcarnitines and acetylcarnitine (C2) but lower palmitoylcarnitine (C16)-to-C2 ratio; a positive relationship between C16 and C2 but negative relationship between carnitine and β-hydroxybutyrate (BOHB); higher branched-chain amino acids (BCAAs) and their ketoacids but lower ketoisocaproate (KIC)-to-Leu, ketomethylvalerate (KMV)-to-Ile, ketoisovalerate (KIV)-to-Val, isovalerylcarnitine-to-KIC+KMV, propionylcarnitine-to-KIV+KMV, KIC+KMV-to-C2, and KIC-to-BOHB ratios; and lower glutamate and 3-methylhistidine. These data suggest that during DKA, patients with KPD resemble patients with T1D in having impaired BCAA catabolism and accelerated fatty acid flux to ketones-a reversal of their distinctive BCAA metabolic defect when stable. The natural history of A-β+ KPD is marked by chronic but varying dysregulation of BCAA metabolism.
© 2021 by the American Diabetes Association.
Figures
References
-
- Banerji MA, Chaiken RL, Huey H, et al. GAD antibody negative NIDDM in adult black subjects with diabetic ketoacidosis and increased frequency of human leukocyte antigen DR3 and DR4. Flatbush diabetes. Diabetes 1994;43:741–745 - PubMed
-
- Maldonado M, Hampe CS, Gaur LK, et al. Ketosis-prone diabetes: dissection of a heterogeneous syndrome using an immunogenetic and beta-cell functional classification, prospective analysis, and clinical outcomes. J Clin Endocrinol Metab 2003;88:5090–5098 - PubMed
-
- Mauvais-Jarvis F, Sobngwi E, Porcher R, et al. Ketosis-prone type 2 diabetes in patients of sub-Saharan African origin: clinical pathophysiology and natural history of beta-cell dysfunction and insulin resistance. Diabetes 2004;53:645–653 - PubMed
-
- Ramos-Román MA, Piñero-Piloña A, Adams-Huet B, Raskin P. Comparison of type 1, type 2, and atypical ketosis-prone diabetes at 4 years of diabetes duration. J Diabetes Complications 2006;20:137–144 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
