

Importance of beta-lactam pharmacokinetics and pharmacodynamics on the recovery of microbial diversity in the airway of persons with cystic fibrosis
- PMID: 34021052
- PMCID: PMC8485129
- DOI: 10.1136/jim-2021-001824
Importance of beta-lactam pharmacokinetics and pharmacodynamics on the recovery of microbial diversity in the airway of persons with cystic fibrosis
Abstract
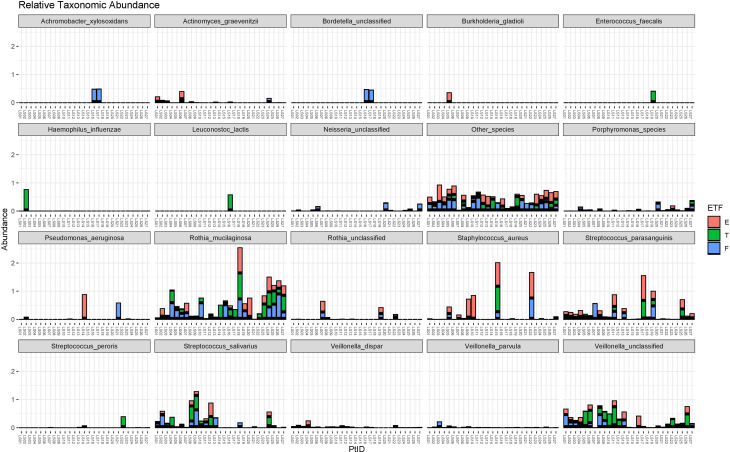
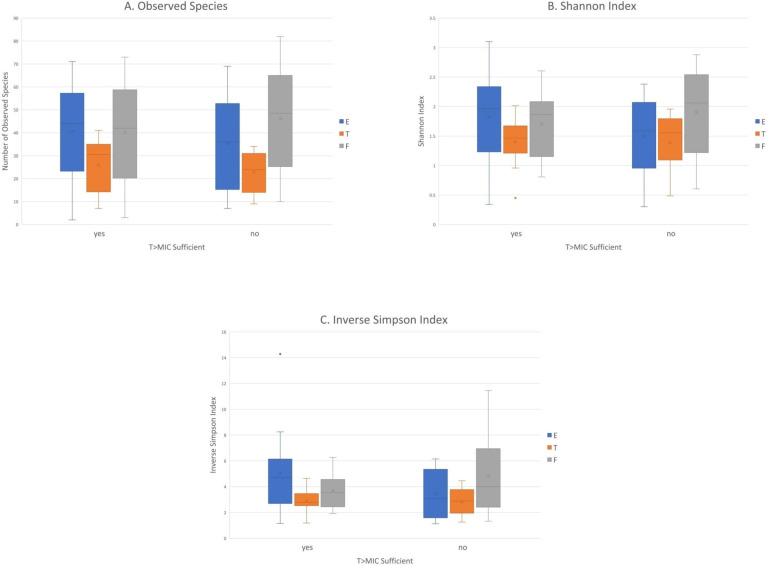
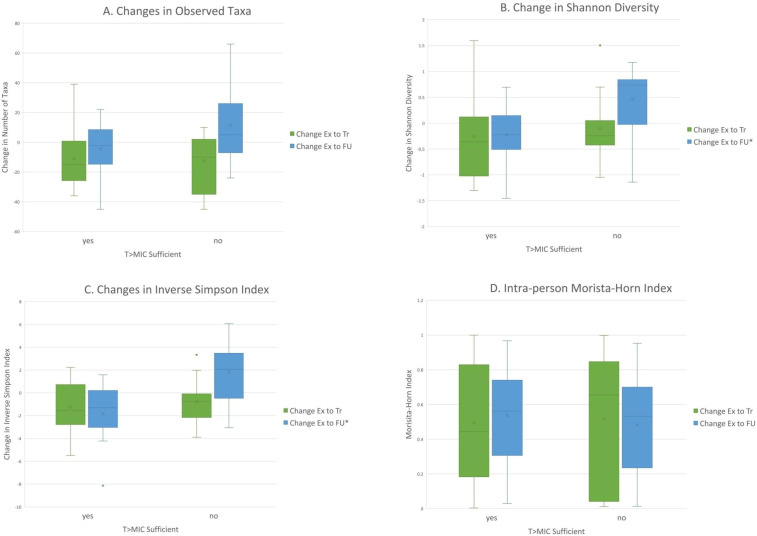
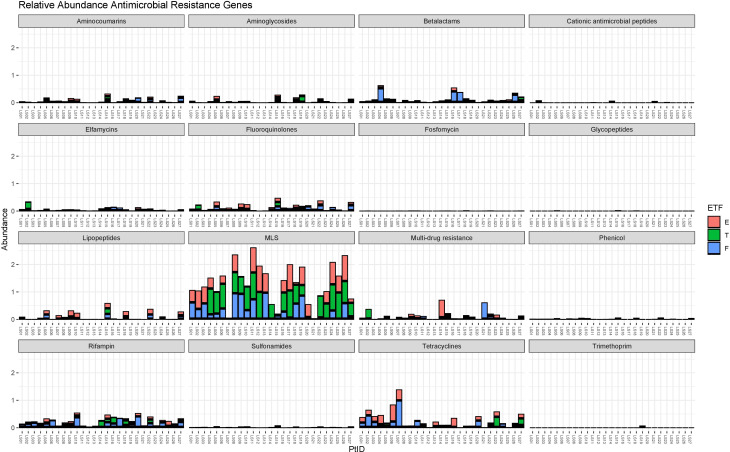
Cystic fibrosis (CF) is a chronic lung disease characterized by acute pulmonary exacerbations (PExs) that are frequently treated with antibiotics. The impact of antibiotics on airway microbial diversity remains a critical knowledge gap. We sought to define the association between beta-lactam pharmacokinetic (PK) and pharmacodynamic target attainment on richness and alpha diversity. Twenty-seven children <18 years of age with CF participated in the prospective study. Airway samples were collected at hospital admission for PEx, end of antibiotic treatment (Tr), and >1 month in follow-up (FU). Metagenomic sequencing was performed to determine richness, alpha diversity, and the presence of antibiotic resistance genes. Free plasma beta-lactam levels were measured, and PK modeling was performed to determine time above the minimum inhibitory concentration (fT>MIC). 52% of study subjects had sufficient fT>MIC for optimal bacterial killing. There were no significant differences in demographics or PEx characteristics, except for F508del homozygosity. No significant differences were noted in richness or alpha diversity at individual time points, and both groups experienced a decrease in richness and alpha diversity at Tr compared with PEx. However, alpha diversity remained decreased at FU compared with PEx in those with sufficient fT>MIC but increased in those with insufficient fT>MIC (Shannon -0.222 vs +0.452, p=0.031, and inverse Simpson -1.376 vs +1.388, p=0.032). Fluoroquinolone resistance was also more frequently detected in those with insufficient fT>MIC (log2 fold change (log2FC) 2.29, p=0.025). These findings suggest sufficient beta-lactam fT>MIC is associated with suppressed recovery of alpha diversity following the antibiotic exposure period.
Keywords: anti-bacterial agents; lung diseases; microbiota.
© American Federation for Medical Research 2021. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Therapeutic beta-lactam dosages and broad-spectrum antibiotics are associated with reductions in microbial richness and diversity in persons with cystic fibrosis.Sci Rep. 2023 Jan 21;13(1):1217. doi: 10.1038/s41598-023-27628-x. Sci Rep. 2023. PMID: 36681756 Free PMC article.
-
Changes in microbiome diversity following beta-lactam antibiotic treatment are associated with therapeutic versus subtherapeutic antibiotic exposure in cystic fibrosis.Sci Rep. 2019 Feb 22;9(1):2534. doi: 10.1038/s41598-019-38984-y. Sci Rep. 2019. PMID: 30796252 Free PMC article.
-
Pharmacokinetic-Pharmacodynamic Target Attainment Analyses To Determine Optimal Dosing of Ceftazidime-Avibactam for the Treatment of Acute Pulmonary Exacerbations in Patients with Cystic Fibrosis.Antimicrob Agents Chemother. 2017 Sep 22;61(10):e00988-17. doi: 10.1128/AAC.00988-17. Print 2017 Oct. Antimicrob Agents Chemother. 2017. PMID: 28784670 Free PMC article. Clinical Trial.
-
Prolonged administration of β-lactam antibiotics - a comprehensive review and critical appraisal.Swiss Med Wkly. 2016 Oct 10;146:w14368. doi: 10.4414/smw.2016.14368. eCollection 2016. Swiss Med Wkly. 2016. PMID: 27731492 Review.
-
Prolonged Versus Intermittent Infusion of β-Lactam Antibiotics: A Systematic Review and Meta-Regression of Bacterial Killing in Preclinical Infection Models.Clin Pharmacokinet. 2020 Oct;59(10):1237-1250. doi: 10.1007/s40262-020-00919-6. Clin Pharmacokinet. 2020. PMID: 32710435
Cited by
-
Perspectives of Therapeutic Drug Monitoring of Biological Agents in Non-Infectious Uveitis Treatment: A Review.Pharmaceutics. 2023 Feb 25;15(3):766. doi: 10.3390/pharmaceutics15030766. Pharmaceutics. 2023. PMID: 36986627 Free PMC article. Review.
-
Using metabolic potential within the airway microbiome as predictors of clinical state in persons with cystic fibrosis.Front Med (Lausanne). 2023 Jan 9;9:1082125. doi: 10.3389/fmed.2022.1082125. eCollection 2022. Front Med (Lausanne). 2023. PMID: 36698799 Free PMC article.
-
Therapeutic beta-lactam dosages and broad-spectrum antibiotics are associated with reductions in microbial richness and diversity in persons with cystic fibrosis.Sci Rep. 2023 Jan 21;13(1):1217. doi: 10.1038/s41598-023-27628-x. Sci Rep. 2023. PMID: 36681756 Free PMC article.
-
Antibiotic resistance in chronic respiratory diseases: from susceptibility testing to the resistome.Eur Respir Rev. 2022 May 25;31(164):210259. doi: 10.1183/16000617.0259-2021. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35613743 Free PMC article. Review.
-
Effects of Therapeutic Antibiotic Exposure on the Oropharyngeal and Fecal Microbiota in Infants With Cystic Fibrosis.Pediatr Pulmonol. 2025 Mar;60(3):e71024. doi: 10.1002/ppul.71024. Pediatr Pulmonol. 2025. PMID: 40042126 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
