

Prevalence of SARS-CoV-2 antibodies in France: results from nationwide serological surveillance
- PMID: 34021152
- PMCID: PMC8140151
- DOI: 10.1038/s41467-021-23233-6
Prevalence of SARS-CoV-2 antibodies in France: results from nationwide serological surveillance
Abstract
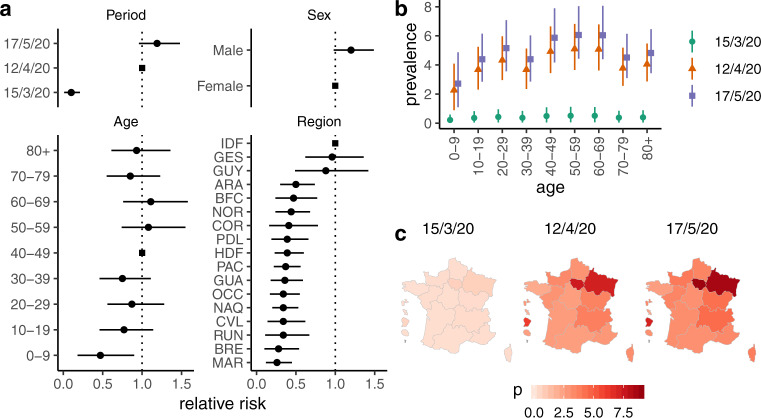
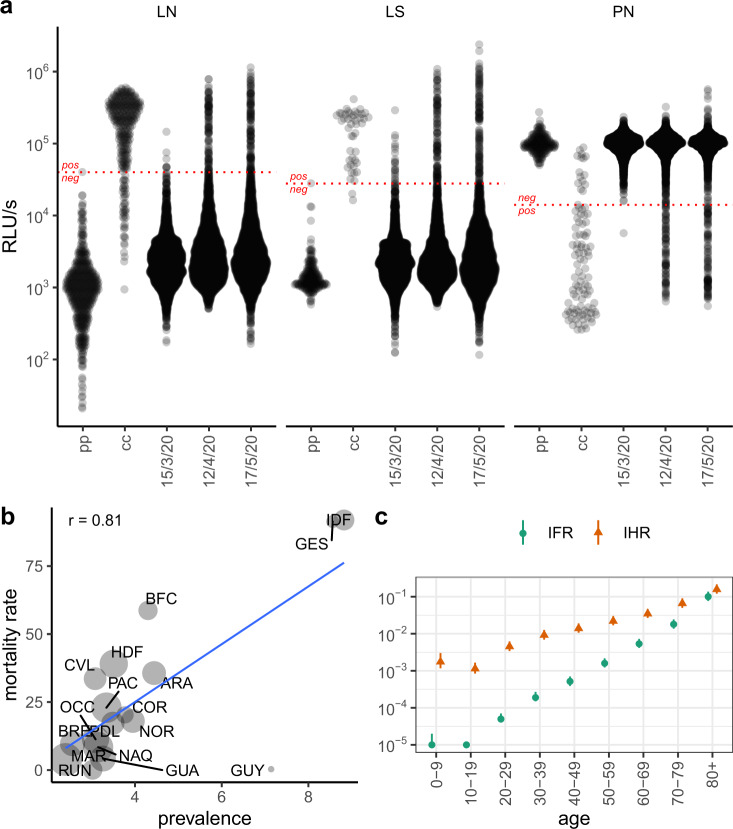
Assessment of the cumulative incidence of SARS-CoV-2 infections is critical for monitoring the course and extent of the COVID-19 epidemic. Here, we report estimated seroprevalence in the French population and the proportion of infected individuals who developed neutralising antibodies at three points throughout the first epidemic wave. Testing 11,000 residual specimens for anti-SARS-CoV-2 IgG and neutralising antibodies, we find nationwide seroprevalence of 0.41% (95% CI: 0.05-0.88) mid-March, 4.14% (95% CI: 3.31-4.99) mid-April and 4.93% (95% CI: 4.02-5.89) mid-May 2020. Approximately 70% of seropositive individuals have detectable neutralising antibodies. Infection fatality rate is 0.84% (95% CI: 0.70-1.03) and increases exponentially with age. These results confirm that the nationwide lockdown substantially curbed transmission and that the vast majority of the French population remained susceptible to SARS-CoV-2 in May 2020. Our study shows the progression of the first epidemic wave and provides a framework to inform the ongoing public health response as viral transmission continues globally.
Conflict of interest statement
S.G. and T.R. declare patents for the proluciferins (hikarazines) synthesis and uses (“Imidazopyrazine derivatives, process for preparation thereof and their uses as luciferins”, EP 3395803/WO 2018197727, 2018), and have applied for a patent that includes claims describing the LuLISA (EP20315224.4) used in this study. F.A. and P.C. have applied for a patent claiming the PNT (“High throughput methods and products for SARS-CoV-2 sero-neutralization assay” US 63/107,896). N.E., M.G., C.D. and S.v.d.W. declare patents pending for the SARS-associated coronavirus diagnostics (“Severe acute respiratory syndrome (SARS)-associated coronavirus diagnostics”, US 10,948,490 B1) related to this study. S.v.d.W. and N.E. declare patents issued (“Use of proteins and peptides coded by the genome of a novel strain of SARS-associated coronavirus” EP 1697507; and “Novel strain of SARS-associated coronavirus and applications thereof” EP1694829) not directly related to this study. S.v.d.W. is a board member (non-financial support) for the International Society for Influenza and other Respiratory Virus Diseases and has a patent application filed (“Methods and reagents for the specific and sensitive detection of SARS-CoV-2”, PCT/EP2020055939 and US16/809,717), not directly related to this study. The other authors declare no competing interests.
Figures
References
-
- Carrat, F. et al. Seroprevalence of SARS-CoV-2 among adults in three regions of France following the lockdown and associated risk factors: a multicohort study. medRxiv10.1101/2020.09.16.20195693 (2020).
-
- Ward, H. et al. Antibody prevalence for SARS-CoV-2 in England following first peak of the pandemic: REACT2 study in 100,000 adults. medRxiv10.1101/2020.08.12.20173690 (2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
