

Pediatric endoscopic pilonidal sinus treatment (PEPSiT): what we learned after a 3-year experience in the pediatric population
- PMID: 34021885
- PMCID: PMC8606398
- DOI: 10.1007/s13304-021-01094-4
Pediatric endoscopic pilonidal sinus treatment (PEPSiT): what we learned after a 3-year experience in the pediatric population
Abstract
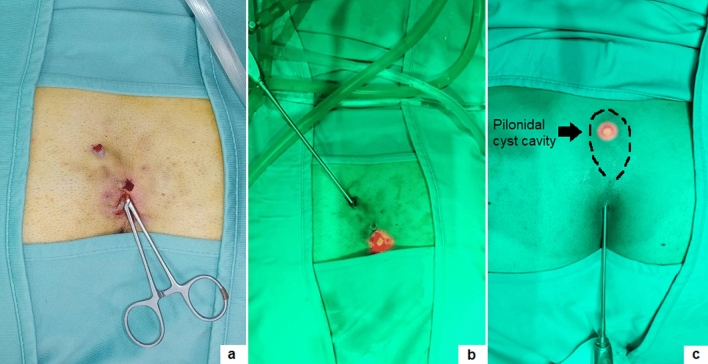
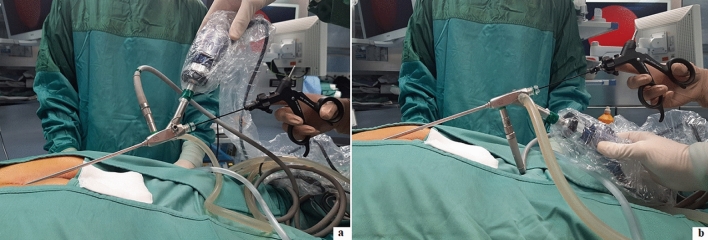
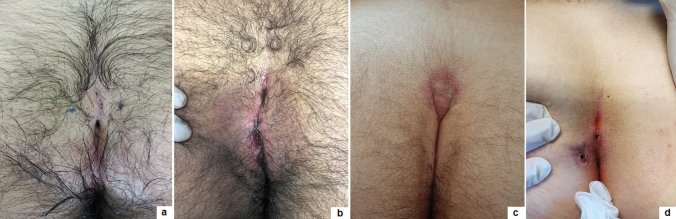
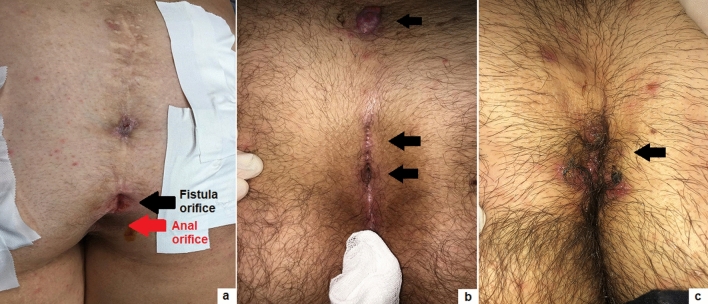
This paper aimed to report a multi-institutional 3-year experience with pediatric endoscopic pilonidal sinus treatment (PEPSiT) and describe tips and tricks of the technique. We retrospectively reviewed all patients < 18 years, with primary or recurrent pilonidal sinus disease (PSD), undergoing PEPSiT in the period 2017-2020. All patients received pre-operative laser therapy, PEPSiT and post-operative dressing and laser therapy. Success rate, healing rate/time, post-operative management, short- and long-term outcome and patient satisfaction were assessed. A total of 152 patients (98 boys) were included. Median patient's age was 17.1 years. Fifteen/152 patients (9.8%) presented a recurrent PSD. All patients resumed full daily activities 1 day after surgery. The post-operative course was painless in 100% of patients (median VAS pain score < 2/10). Patient satisfaction was excellent (median score 4.8). The median follow-up was 12.8 months (range 1-36). Complete healing in 8 weeks was achieved in 145/152 (95.4%) and the median healing time was 24.6 days (range 16-31). We reported post-operatively immediate Clavien grade 2 complications (3 oedema, 2 burns) in 5/152 (3.3%) and delayed Clavien grade 2 complications (3 granulomas, 8 wound infections) in 11/152 (7.2%). Disease recurrence occurred in 7/152 (4.6%), who were re-operated using PEPSiT. PEPSiT should be considered the standard of care for surgical treatment of PSD in children and teenagers. PEPSiT is technically easy, with short and painless post-operative course and low recurrence rate (4.6%). Standardized treatment protocol, correct patient enrollment and information, and intensive follow-up are key points for the success of the procedure.
Keywords: Dressing; Fistuloscope; Laser; PEPSiT; Technique; Teenagers.
© 2021. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Figures



Similar articles
-
Pediatric endoscopic pilonidal sinus treatment (PEPSiT): report of a multicentric national study on 294 patients.Updates Surg. 2023 Sep;75(6):1625-1631. doi: 10.1007/s13304-023-01508-5. Epub 2023 May 5. Updates Surg. 2023. PMID: 37145226 Free PMC article.
-
Pediatric Endoscopic Pilonidal Sinus Treatment (PEPSiT) in Children With Pilonidal Sinus Disease: Tips and Tricks and New Structurated Protocol.Front Pediatr. 2020 Jun 24;8:345. doi: 10.3389/fped.2020.00345. eCollection 2020. Front Pediatr. 2020. PMID: 32671004 Free PMC article.
-
Pediatric Endoscopic Pilonidal Sinus Treatment: An Effective Procedure for Children with Recurrent Pilonidal Sinus Disease After Failed Open Surgery.J Laparoendosc Adv Surg Tech A. 2019 Jul;29(7):981-986. doi: 10.1089/lap.2019.0031. Epub 2019 Apr 13. J Laparoendosc Adv Surg Tech A. 2019. PMID: 30985239
-
Quality of life of pediatric patients operated for pilonidal sinus disease.Eur J Pediatr. 2023 Jan;182(1):25-30. doi: 10.1007/s00431-022-04678-3. Epub 2022 Nov 8. Eur J Pediatr. 2023. PMID: 36348071 Free PMC article. Review.
-
Outcomes of Pediatric Endoscopic Pilonidal Sinus Treatment: A Systematic Review.Eur J Pediatr Surg. 2024 Aug;34(4):294-300. doi: 10.1055/s-0043-1771224. Epub 2023 Jul 26. Eur J Pediatr Surg. 2024. PMID: 37494954
Cited by
-
Long-term results of EPSiT in children and adolescents: still the right way to go.Pediatr Surg Int. 2022 Sep;38(9):1257-1261. doi: 10.1007/s00383-022-05162-7. Epub 2022 Jul 2. Pediatr Surg Int. 2022. PMID: 35779104
-
Endoscopic Pilonidal Sinus Treatment: Preliminary Results, Learning Curve and Comparison with Standard Open Approach.Children (Basel). 2023 Jun 15;10(6):1063. doi: 10.3390/children10061063. Children (Basel). 2023. PMID: 37371294 Free PMC article.
-
Endoscopic approach to complex or recurrent pilonidal sinus: A retrospective analysis.Int Wound J. 2023 Apr;20(4):1212-1218. doi: 10.1111/iwj.13980. Epub 2022 Oct 21. Int Wound J. 2023. PMID: 36271666 Free PMC article.
-
The role of alginate dressings in wound healing and quality of life after pilonidal sinus resection: A randomised controlled trial.Int Wound J. 2022 Oct;19(6):1528-1538. doi: 10.1111/iwj.13752. Epub 2022 Jan 18. Int Wound J. 2022. PMID: 35043571 Free PMC article. Clinical Trial.
-
Pediatric endoscopic pilonidal sinus treatment: lessons learned after 100 consecutive cases.Tech Coloproctol. 2024 Dec 10;29(1):14. doi: 10.1007/s10151-024-03049-4. Tech Coloproctol. 2024. PMID: 39656288
References
-
- Esposito C, Izzo S, Turrà F, Cerulo M, Severino G, Settimi A, Iannazzone M, Masieri L, Cortese G, Escolino M. Pediatric endoscopic pilonidal sinus treatment, a revolutionary technique to adopt in children with pilonidal sinus fistulas: our preliminary experience. J Laparoendosc Adv Surg Tech A. 2018;28(3):359–363. doi: 10.1089/lap.2017.0246. - DOI - PubMed
-
- Pini Prato A, Mazzola C, Mattioli G, Escolino M, Esposito C, D'Alessio A, Abati LC, Leonelli L, Carlini C, Rotundi F, Meinero PC. Preliminary report on endoscopic pilonidal sinus treatment in children: results of a multicentric series. Pediatr Surg Int. 2018;34(6):687–692. doi: 10.1007/s00383-018-4262-0. - DOI - PubMed
-
- Sequeira JB, Coelho A, Marinho AS, Bonet B, Carvalho F, Moreira-Pinto J. Endoscopic pilonidal sinus treatment versus total excision with primary closure for sacrococcygeal pilonidal sinus disease in the pediatric population. J Pediatr Surg. 2018;53(10):2003–2007. doi: 10.1016/j.jpedsurg.2018.02.094. - DOI - PubMed
-
- Esposito C, Gargiulo F, Izzo S, Cerulo M, Del Conte F, Severino G, Escolino M. Pediatric endoscopic pilonidal sinus treatment: an effective procedure for children with recurrent pilonidal sinus disease after failed open surgery. J Laparoendosc Adv Surg Tech A. 2019;29(7):981–986. doi: 10.1089/lap.2019.0031. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
