

Innate immune and inflammatory responses to SARS-CoV-2: Implications for COVID-19
- PMID: 34022154
- PMCID: PMC8126603
- DOI: 10.1016/j.chom.2021.05.004
Innate immune and inflammatory responses to SARS-CoV-2: Implications for COVID-19
Abstract
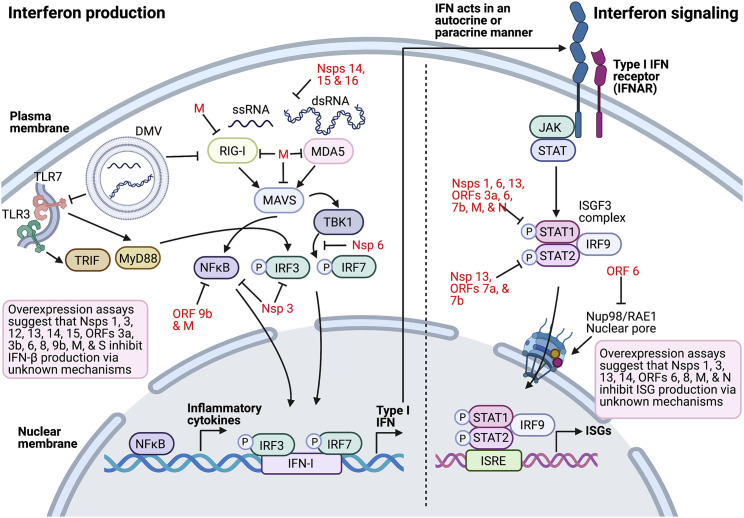
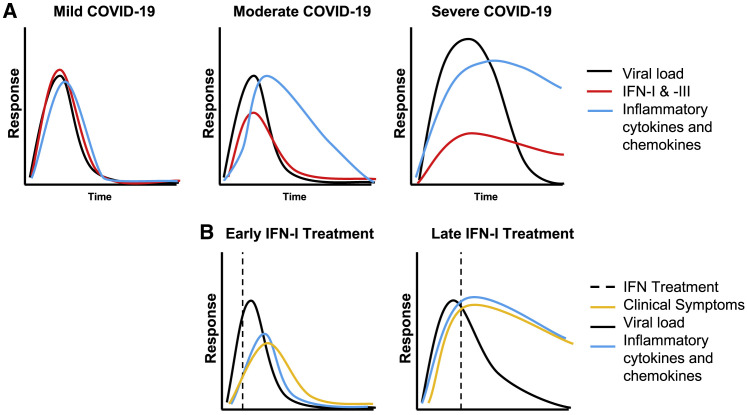
COVID-19 can result in severe disease characterized by significant immunopathology that is spurred by an exuberant, yet dysregulated, innate immune response with a poor adaptive response. A limited and delayed interferon I (IFN-I) and IFN-III response results in exacerbated proinflammatory cytokine production and in extensive cellular infiltrates in the respiratory tract, resulting in lung pathology. The development of effective therapeutics for patients with severe COVID-19 depends on our understanding of the pathological elements of this unbalanced innate immune response. Here, we review the mechanisms by which SARS-CoV-2 both activates and antagonizes the IFN and inflammatory response following infection, how a dysregulated cytokine and cellular response contributes to immune-mediated pathology in COVID-19, and therapeutic strategies that target elements of the innate response.
Keywords: SARS-CoV-2; coronavirus; cytokines; immune antagonism; immune evasion; inflammatory; innate immunity; interferon.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
References
-
- Angus D.C., Derde L., Al-Beidh F., Annane D., Arabi Y., Beane A., van Bentum-Puijk W., Berry L., Bhimani Z., Bonten M., et al. Writing Committee for the REMAP-CAP Investigators Effect of Hydrocortisone on Mortality and Organ Support in Patients With Severe COVID-19: The REMAP-CAP COVID-19 Corticosteroid Domain Randomized Clinical Trial. JAMA. 2020;324:1317–1329. - PMC - PubMed
-
- Arabi Y.M., Asiri A.Y., Assiri A.M., Balkhy H.H., Al Bshabshe A., Al Jeraisy M., Mandourah Y., Azzam M.H.A., Bin Eshaq A.M., Al Johani S., et al. Saudi Critical Care Trials Group Interferon Beta-1b and Lopinavir-Ritonavir for Middle East Respiratory Syndrome. N. Engl. J. Med. 2020;383:1645–1656. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
