

Risks of recurrent stroke and all serious vascular events after spontaneous intracerebral haemorrhage: pooled analyses of two population-based studies
- PMID: 34022170
- PMCID: PMC8134058
- DOI: 10.1016/S1474-4422(21)00075-2
Risks of recurrent stroke and all serious vascular events after spontaneous intracerebral haemorrhage: pooled analyses of two population-based studies
Erratum in
-
Correction to Lancet Neurol 2021; 20: 437-47.Lancet Neurol. 2021 Aug;20(8):e5. doi: 10.1016/S1474-4422(21)00185-X. Epub 2021 Jun 9. Lancet Neurol. 2021. PMID: 34118201 Free PMC article. No abstract available.
Abstract
Background: Patients with stroke due to spontaneous (non-traumatic) intracerebral haemorrhage (ICH) are at risk of recurrent ICH, ischaemic stroke, and other serious vascular events. We aimed to analyse these risks in population-based studies and compare them with the risks in RESTART, which assessed antiplatelet therapy after ICH.
Methods: We pooled individual patient data from two prospective, population-based inception cohort studies of all patients with an incident firs-in-a-lifetime ICH in Oxfordshire, England (Oxford Vascular Study; April 1, 2002, to Sept 28, 2018) and Lothian, Scotland, UK (Lothian Audit of the Treatment of Cerebral Haemorrhage; June 1, 2010, to May 31, 2013). We quantified the absolute and relative risks of recurrent ICH, ischaemic stroke, or any serious vascular event (non-fatal stroke, non-fatal myocardial infarction, or vascular death), stratified by ICH location (lobar vs non-lobar) and comorbid atrial fibrillation (AF). We compared pooled event rates with those after allocation to avoid antiplatelet therapy in RESTART.
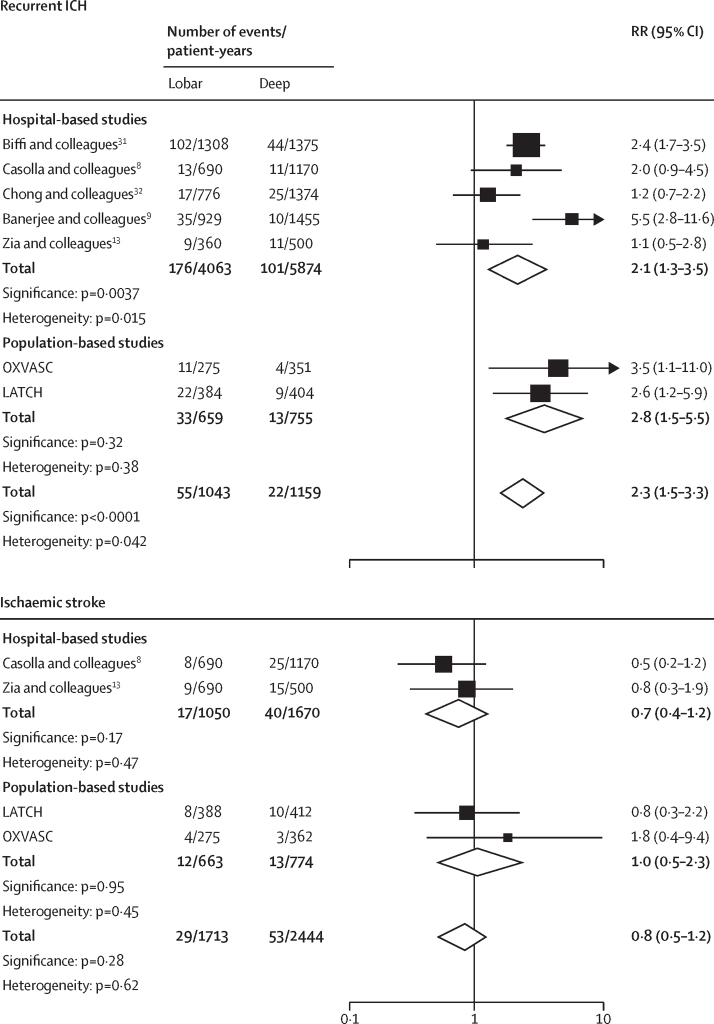
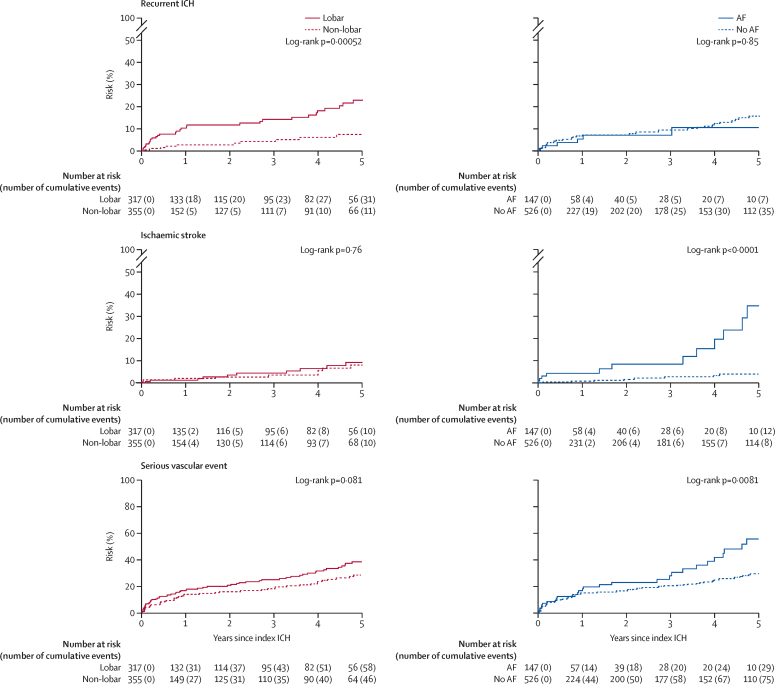
Findings: Among 674 patients (mean age 74·7 years [SD 12·6], 320 [47%] men) with 1553 person-years of follow-up, 46 recurrent ICHs (event rate 3·2 per 100 patient-years, 95% CI 2·0-5·1) and 25 ischaemic strokes (1·7 per 100 patient-years, 0·8-3·3) were reported. Patients with lobar ICH (n=317) had higher risk of recurrent ICH (5·1 per 100 patient-years, 95% CI 3·6-7·2) than patients with non-lobar ICH (n=355; 1·8 per 100 patient-years, 1·0-3·3; hazard ratio [HR] 3·2, 95% CI 1·6-6·3; p=0·0010), but there was no evidence of a difference in the risk of ischaemic stroke (1·8 per 100 patient-years, 1·0-3·2, vs 1·6 per 100 patient-years, 0·6-4·4; HR 1·1, 95% CI 0·5-2·8). Conversely, there was no evidence of a difference in recurrent ICH rate in patients with AF (n=147; 3·3 per 100 patient-years, 95% CI 1·0-10·7) compared with those without (n=526; 3·2 per 100 patient-years, 2·2-4·7; HR 0·9, 95% CI 0·4-2·1), but the risk of ischaemic stroke was higher with AF (6·3 per 100 patient-years, 3·7-10·9, vs 0·7 per 100 patient-years, 0·1-5·6; HR 8·2, 3·3-20·3; p<0·0001), resulting in patients with AF having a higher risk of all serious vascular events than patients without AF (15·5 per 100 patient-years, 10·0-24·1, vs 6·8 per 100 patient-years, 3·6-12·5; HR 1·78, 95% CI 1·16-2·74; p=0·0090). Only for patients with lobar ICH without comorbid AF was the risk of recurrent ICH greater than the risk of ischaemic stroke (5·2 per 100 patient-years, 95% CI 3·6-7·5, vs 0·9 per 100 patient-years, 0·2-4·8; p=0·00034). Comparing data from the pooled population-based studies with that from patients allocated to not receive antiplatelet therapy in RESTART, there was no evidence of a difference in the rate of recurrent ICH (3·5 per 100 patient-years, 95% CI 1·9-6·0, vs 4·4 per 100 patient-years, 2·6-6·1) or ischaemic stroke (3·4 per 100 patient-years, 1·9-5·9, vs 5·3 per 100 patient-years, 3·3-7·2).
Interpretation: The risks of recurrent ICH, ischaemic stroke, and all serious vascular events after ICH differ by ICH location and comorbid AF. These data enable risk stratification of patients in clinical practice and ongoing randomised trials.
Funding: UK Medical Research Council, Stroke Association, British Heart Foundation, Wellcome Trust, and the National Institute for Health Research Oxford Biomedical Research Centre.
Trial registration: ClinicalTrials.gov NCT02699645 NCT03863665 NCT04522102 NCT03996772 NCT03950076 NCT02565693 NCT03186729 NCT03243175 NCT03153150 NCT03996772 NCT03950076.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TJM reports grants from the British Heart Foundation clinical research training fellowship outside the submitted work. MAR and JJML report grants from The Wellcome Trust during the conduct of the study. RA-SS reports grants from the Medical Research Council during the conduct of the study. All other authors declare no competing interests.
Figures
Comment in
-
Towards individualised secondary prevention after intracerebral haemorrhage.Lancet Neurol. 2021 Jun;20(6):411-413. doi: 10.1016/S1474-4422(21)00130-7. Lancet Neurol. 2021. PMID: 34022160 No abstract available.
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. - PubMed
-
- Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the Global Burden of Disease study 2017. Neuroepidemiology. 2020;54:171–179. - PubMed
-
- Samarasekera N, Fonville A, Lerpiniere C. Influence of intracerebral hemorrhage location on incidence, characteristics, and outcome: population-based study. Stroke. 2015;46:361–368. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
