

Interferon-gamma release assay levels and risk of progression to active tuberculosis: a systematic review and dose-response meta-regression analysis
- PMID: 34022827
- PMCID: PMC8141158
- DOI: 10.1186/s12879-021-06141-4
Interferon-gamma release assay levels and risk of progression to active tuberculosis: a systematic review and dose-response meta-regression analysis
Abstract
Background: Identifying and treating individuals with high risk of progression from latent tuberculosis infection to active tuberculosis (TB) disease is critical for eliminating the disease. We aimed to conduct a systematic review and meta-regression analysis to quantify the dose-response relationship between interferon-gamma release assay (IGRA) levels and the risk of progression to active TB.
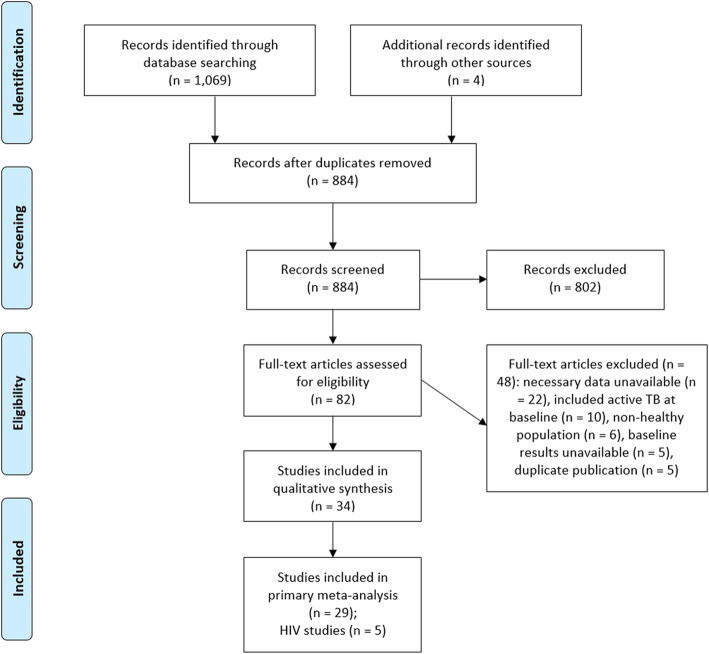
Methods: We searched PubMed and Embase from 1 January 2001 to 10 May 2020 for longitudinal studies that reported the risk of progression from latent to active TB as a function of baseline IGRA values. We used a novel Bayesian meta-regression method to pool effect sizes from included studies and generate a continuous dose-response risk curve. Our modeling framework enabled us to incorporate random effects across studies, and include data with different IGRA ranges across studies. The quality of included studies were assessed using the Newcastle-Ottawa scale (NOS).
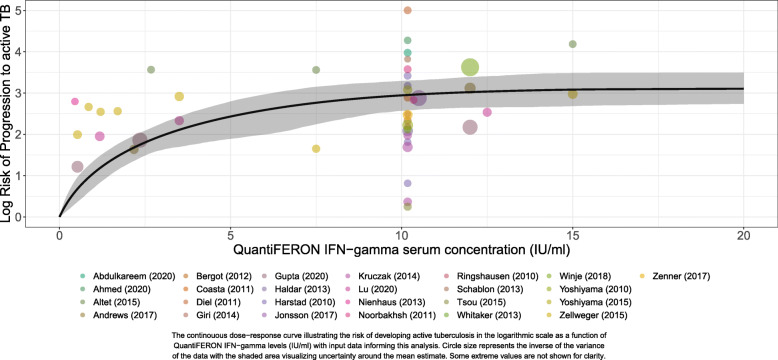
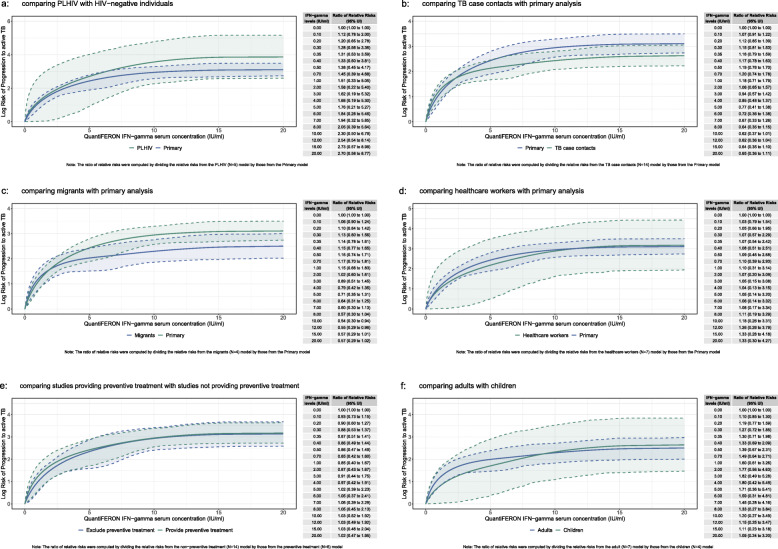
Results: We included 34 studies representing 581,956 person-years of follow-up with a total of 788 incident cases of TB in the meta-regression analysis. Higher levels of interferon-gamma were associated with increased risk of progression to active tuberculosis. In the dose-response curve, the risk increased sharply between interferon-gamma levels 0 and 5 IU/ml, after which the risk continued to increase moderately but at a slower pace until reaching about 15 IU/ml where the risk levels off. Compared to 0 IU/ml, the relative risk of progression to active TB among those with interferon-gamma levels of 0.35, 1, 5, 10, 15, and 20 IU/ml were: 1.64 (1.28-2.08), 2.90 (2.02-3.88), 11.38 (6.64-16.38), 19.00 (13.08-26.90), 21.82 (14.65-32.57), and 22.31 (15.43-33.00), respectively. The dose-response relationship remains consistent when limiting the analysis to studies that scored highest in the NOS.
Conclusion: The current practice of dichotomizing IGRA test results simplifies the TB infection disease continuum. Evaluating IGRA test results over a continuous scale could enable the identification of individuals at greatest risk of progression to active TB.
Keywords: Active tuberculosis; Dose-response meta-regression; IGRA; Latent tuberculosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222. doi: 10.1016/S0140-6736(20)30925-9. - DOI - PMC - PubMed
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
