

Time controlled adaptive ventilation™ as conservative treatment of destroyed lung: an alternative to lung transplantation
- PMID: 34022829
- PMCID: PMC8140588
- DOI: 10.1186/s12890-021-01545-z
Time controlled adaptive ventilation™ as conservative treatment of destroyed lung: an alternative to lung transplantation
Abstract
Background: Acute respiratory distress syndrome (ARDS) often requires controlled ventilation, yielding high mechanical power and possibly further injury. Veno-venous extracorporeal membrane oxygenation (VV-ECMO) can be used as a bridge to recovery, however, if this fails the end result is destroyed lung parenchyma. This condition is fatal and the only remaining alternative is lung transplantation. In the case study presented in this paper, lung transplantation was not an option given the critically ill state and the presence of HLA antibodies. Airway pressure release ventilation (APRV) may be valuable in ARDS, but APRV settings recommended in various patient and clinical studies are inconsistent. The Time Controlled Adaptive Ventilation (TCAV™) method is the most studied technique to set and adjust the APRV mode and uses an extended continuous positive airway pressure (CPAP) Phase in combination with a very brief Release Phase. In addition, the TCAV™ method settings are personalized and adaptive based on changes in lung pathophysiology. We used the TCAV™ method in a case of severe ARDS, which enabled us to open, stabilize and slowly heal the severely damaged lung parenchyma.
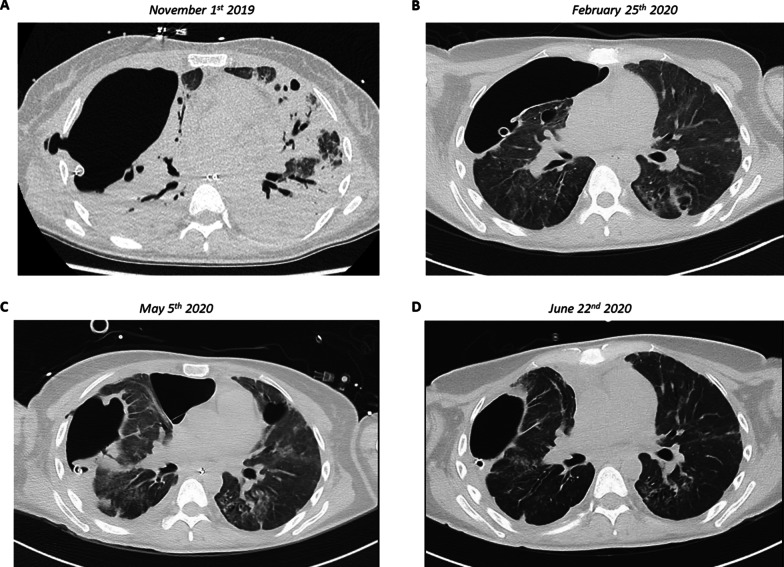
Case presentation: A 43-year-old woman presented with Staphylococcus Aureus necrotizing pneumonia. Progressive respiratory failure necessitated invasive mechanical ventilation and VV-ECMO. Mechanical ventilation (MV) was ultimately discontinued because lung protective settings resulted in trivial tidal volumes. She was referred to our academic transplant center for bilateral lung transplantation after the remaining infection had been cleared. We initiated the TCAV™ method in order to stabilize the lung parenchyma and to promote tissue recovery. This strategy was challenged by the presence of a large bronchopleural fistula, however, APRV enabled weaning from VV-ECMO and mechanical ventilation. After two months, following nearly complete surgical closure of the remaining bronchopleural fistulas, the patient was readmitted to ICU where she had early postoperative complications. Since other ventilation modes resulted in significant atelectasis and hypercapnia, APRV was restarted. The patient was then again weaned from MV.
Conclusions: The TCAV™ method can be useful to wean challenging patients with severe ARDS and might contribute to lung recovery. In this particular case, a lung transplantation was circumvented.
Keywords: Acute respiratory distress syndrome; Bronchopleural fistula; Destroyed lung; Lung protective ventilation; Time-controlled adaptive ventilation; Veno-venous extracorporeal membrane oxygenation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome.Intensive Care Med. 2017 Nov;43(11):1648-1659. doi: 10.1007/s00134-017-4912-z. Epub 2017 Sep 22. Intensive Care Med. 2017. PMID: 28936695 Free PMC article.
-
Early pathophysiology-driven airway pressure release ventilation versus low tidal volume ventilation strategy for patients with moderate-severe ARDS: study protocol for a randomized, multicenter, controlled trial.BMC Pulm Med. 2024 May 23;24(1):252. doi: 10.1186/s12890-024-03065-y. BMC Pulm Med. 2024. PMID: 38783268 Free PMC article.
-
Does Earlier Cannulation With Veno-Venous Extracorporeal Membrane Oxygenation in Adult Patients With Acute Respiratory Distress Syndrome Decrease Duration of Artificial Mechanical Ventilation?J Dr Nurs Pract. 2020 Jul 1;13(2):148-155. doi: 10.1891/JDNP-D-19-00059. Epub 2020 Jul 2. J Dr Nurs Pract. 2020. PMID: 32817504
-
Time-Controlled Adaptive Ventilation (TCAV): a personalized strategy for lung protection.Respir Res. 2024 Jan 18;25(1):37. doi: 10.1186/s12931-023-02615-y. Respir Res. 2024. PMID: 38238778 Free PMC article. Review.
-
First Stabilize and then Gradually Recruit: A Paradigm Shift in Protective Mechanical Ventilation for Acute Lung Injury.J Clin Med. 2023 Jul 12;12(14):4633. doi: 10.3390/jcm12144633. J Clin Med. 2023. PMID: 37510748 Free PMC article. Review.
Cited by
-
Future directions in ventilator-induced lung injury associated cognitive impairment: a new sight.Front Physiol. 2023 Dec 18;14:1308252. doi: 10.3389/fphys.2023.1308252. eCollection 2023. Front Physiol. 2023. PMID: 38164198 Free PMC article. Review.
-
Inconsistent Methods Used to Set Airway Pressure Release Ventilation in Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Regression Analysis.J Clin Med. 2024 May 3;13(9):2690. doi: 10.3390/jcm13092690. J Clin Med. 2024. PMID: 38731219 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
