

The effect of community-driven larval source management and house improvement on malaria transmission when added to the standard malaria control strategies in Malawi: a cluster-randomized controlled trial
- PMID: 34022912
- PMCID: PMC8140568
- DOI: 10.1186/s12936-021-03769-0
The effect of community-driven larval source management and house improvement on malaria transmission when added to the standard malaria control strategies in Malawi: a cluster-randomized controlled trial
Abstract
Background: Current standard interventions are not universally sufficient for malaria elimination. The effects of community-based house improvement (HI) and larval source management (LSM) as supplementary interventions to the Malawi National Malaria Control Programme (NMCP) interventions were assessed in the context of an intensive community engagement programme.
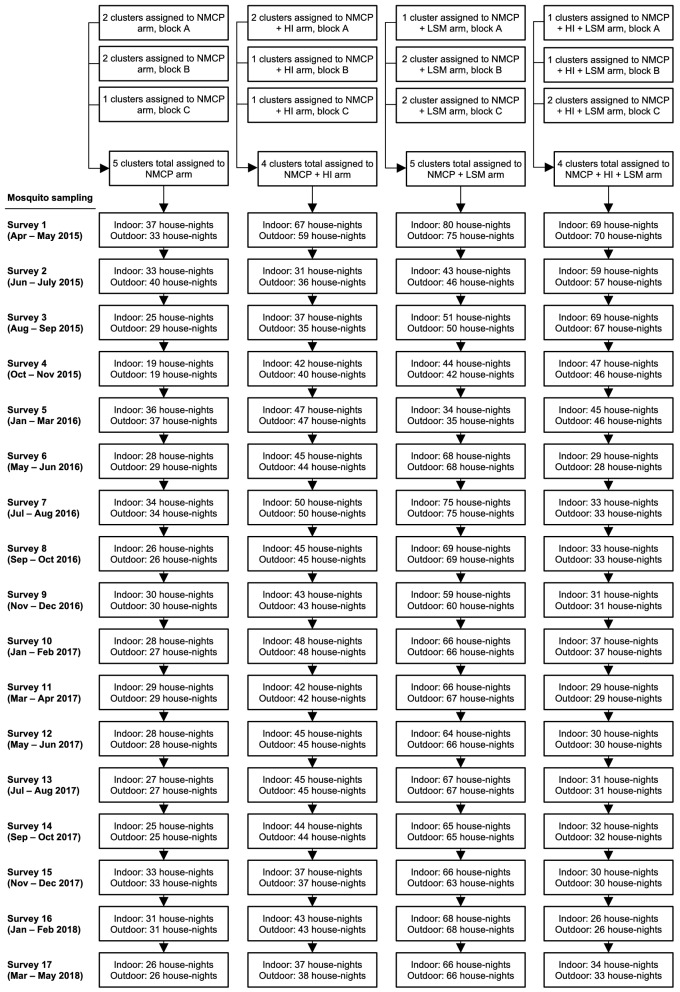
Methods: The study was a two-by-two factorial, cluster-randomized controlled trial in Malawi. Village clusters were randomly assigned to four arms: a control arm; HI; LSM; and HI + LSM. Malawi NMCP interventions and community engagement were used in all arms. Household-level, cross-sectional surveys were conducted on a rolling, 2-monthly basis to measure parasitological and entomological outcomes over 3 years, beginning with one baseline year. The primary outcome was the entomological inoculation rate (EIR). Secondary outcomes included mosquito density, Plasmodium falciparum prevalence, and haemoglobin levels. All outcomes were assessed based on intention to treat, and comparisons between trial arms were conducted at both cluster and household level.
Results: Eighteen clusters derived from 53 villages with 4558 households and 20,013 people were randomly assigned to the four trial arms. The mean nightly EIR fell from 0.010 infectious bites per person (95% CI 0.006-0.015) in the baseline year to 0.001 (0.000, 0.003) in the last year of the trial. Over the full trial period, the EIR did not differ between the four trial arms (p = 0.33). Similar results were observed for the other outcomes: mosquito density and P. falciparum prevalence decreased over 3 years of sampling, while haemoglobin levels increased; and there were minimal differences between the trial arms during the trial period.
Conclusions: In the context of high insecticide-treated bed net use, neither community-based HI, LSM, nor HI + LSM contributed to further reductions in malaria transmission or prevalence beyond the reductions observed over two years across all four trial arms. This was the first trial, as far as the authors are aware, to test the potential complementary impact of LSM and/or HI beyond levels achieved by standard interventions. The unexpectedly low EIR values following intervention implementation indicated a promising reduction in malaria transmission for the area, but also limited the usefulness of this outcome for measuring differences in malaria transmission among the trial arms. Trial registration PACTR, PACTR201604001501493, Registered 3 March 2016, https://pactr.samrc.ac.za/ .
Keywords: Cluster randomised trial; Community engagement; House improvement; Larval source management; Malaria.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- WHO. World malaria report 2015. Geneva, World Health Organization; 2015.
-
- WHO. World malaria report 2018. Geneva, World Health Organization; 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
