

Mechanical circulatory support for refractory out-of-hospital cardiac arrest: a Danish nationwide multicenter study
- PMID: 34022934
- PMCID: PMC8141159
- DOI: 10.1186/s13054-021-03606-5
Mechanical circulatory support for refractory out-of-hospital cardiac arrest: a Danish nationwide multicenter study
Abstract
Background: Mechanical circulatory support (MCS) with either extracorporeal membrane oxygenation or Impella has shown potential as a salvage therapy for patients with refractory out-of-hospital cardiac arrest (OHCA). The objective of this study was to describe the gradual implementation, survival and adherence to the national consensus with respect to use of MCS for OHCA in Denmark, and to identify factors associated with outcome.
Methods: This retrospective, observational cohort study included patients receiving MCS for OHCA at all tertiary cardiac arrest centers (n = 4) in Denmark between July 2011 and December 2020. Logistic regression and Kaplan-Meier survival analysis were used to determine association with outcome. Outcome was presented as survival to hospital discharge with good neurological outcome, 30-day survival and predictors of 30-day mortality.
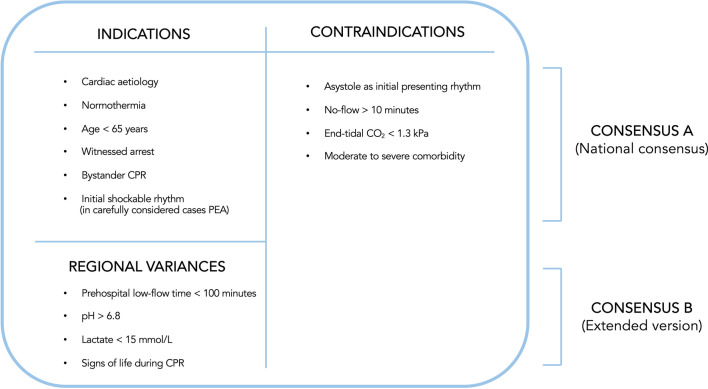
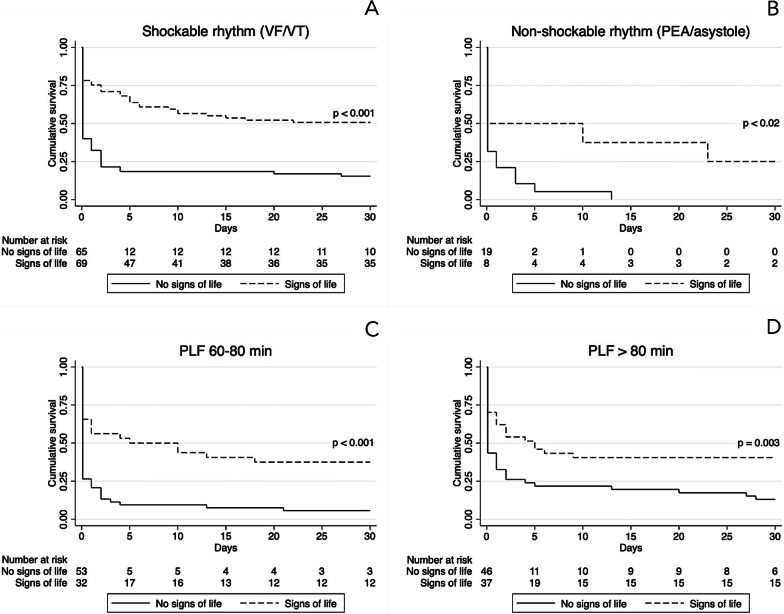
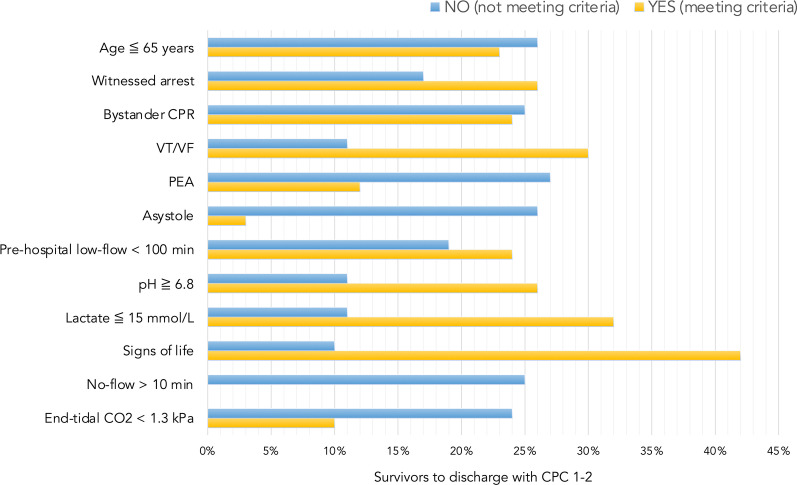
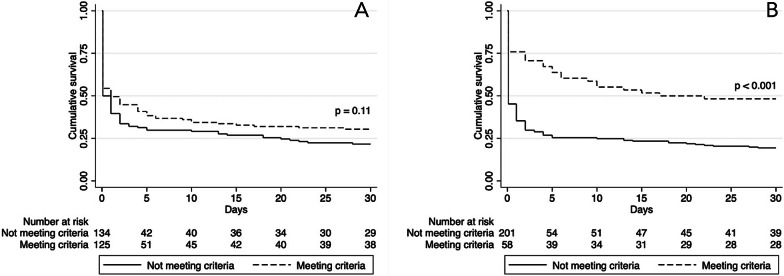
Results: A total of 259 patients were included in the study. Thirty-day survival was 26%. Sixty-five (25%) survived to hospital discharge and a good neurological outcome (Glasgow-Pittsburgh Cerebral Performance Categories 1-2) was observed in 94% of these patients. Strict adherence to the national consensus showed a 30-day survival rate of 30% compared with 22% in patients violating one or more criteria. Adding criteria to the national consensus such as signs of life during cardiopulmonary resuscitation (CPR), pre-hospital low-flow < 100 min, pH > 6.8 and lactate < 15 mmol/L increased the survival rate to 48%, but would exclude 58% of the survivors from the current cohort. Logistic regression identified asystole (RR 1.36, 95% CI 1.18-1.57), pulseless electrical activity (RR 1.20, 95% CI 1.03-1.41), initial pH < 6.8 (RR 1.28, 95% CI 1.12-1.46) and lactate levels > 15 mmol/L (RR 1.16, 95% CI 1.16-1.53) as factors associated with increased risk of 30-day mortality. Patients presenting signs of life during CPR had reduced risk of 30-day mortality (RR 0.63, 95% CI 0.52-0.76).
Conclusions: A high survival rate with a good neurological outcome was observed in this Danish population of patients treated with MCS for OHCA. Stringent patient selection for MCS may produce higher survival rates but potentially withholds life-saving treatment in a significant proportion of survivors.
Keywords: Cardiopulmonary resuscitation; Extracorporeal membrane oxygenation; Impella; Mechanical circulatory support; Out-of-hospital cardiac arrest.
Conflict of interest statement
Dr. Stengaard reports speaker’s fees from Rosche Diagnostics, outside the submitted work. Dr. Møller reports personal fees and grants from Orion Pharma, Novartis, Astra Zeneca, Abbott and Abiomed and served at scientific advisory board for Boehringer Ingelheim, outside the submitted work. Dr. Freeman reports grants from St. Jude and Astra Zeneca and personal fees from Meril Lifesciences and Edwards Lifesciences, outside the submitted work. Dr. Hassager reports grants from the Lundbeck Foundation and speaker’s honoraria from Abiomed, outside the submitted work. Dr. Kjaergaard reports non-financial participation in the advisory board for the CoCa Trial. Dr. Terkelsen is supported by an unrestricted research grant from the Danish Heart Foundation. The remaining authors have no conflicts of interest to declare.
Figures
References
-
- Grasner JT, Wnent J, Herlitz J, Perkins GD, Lefering R, Tjelmeland I, Koster RW, Masterson S, Rossell-Ortiz F, Maurer H, Bottiger BW, Moertl M, Mols P, Alihodzic H, Hadzibegovic I, Ioannides M, Truhlar A, Wissenberg M, Salo A, Escutnaire J, Nikolaou N, Nagy E, Jonsson BS, Wright P, Semeraro F, Clarens C, Beesems S, Cebula G, Correia VH, Cimpoesu D, Raffay V, Trenkler S, Markota A, Stromsoe A, Burkart R, Booth S, Bossaert L. Survival after out-of-hospital cardiac arrest in Europe: results of the EuReCa TWO study. Resuscitation. 2020;148:218–226. doi: 10.1016/j.resuscitation.2019.12.042. - DOI - PubMed
-
- Haneya A, Philipp A, Diez C, Schopka S, Bein T, Zimmermann M, Lubnow M, Luchner A, Agha A, Hilker M, Hirt S, Schmid C, Muller T. A 5-year experience with cardiopulmonary resuscitation using extracorporeal life support in non-postcardiotomy patients with cardiac arrest. Resuscitation. 2012;83:1331–1337. doi: 10.1016/j.resuscitation.2012.07.009. - DOI - PubMed
-
- Sakamoto T, Morimura N, Nagao K, Asai Y, Yokota H, Nara S, Hase M, Tahara Y, Atsumi T and Group S-JS Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with out-of-hospital cardiac arrest: a prospective observational study. Resuscitation. 2014;85:762–768. doi: 10.1016/j.resuscitation.2014.01.031. - DOI - PubMed
-
- Fjolner J, Greisen J, Jorgensen MR, Terkelsen CJ, Ilkjaer LB, Hansen TM, Eiskjaer H, Christensen S, Gjedsted J. Extracorporeal cardiopulmonary resuscitation after out-of-hospital cardiac arrest in a Danish health region. Acta Anaesthesiol Scand. 2017;61:176–185. doi: 10.1111/aas.12843. - DOI - PubMed
-
- Dennis M, McCanny P, D'Souza M, Forrest P, Burns B, Lowe DA, Gattas D, Scott S, Bannon P, Granger E, Pye R, Totaro R, Sydney ERIG. Extracorporeal cardiopulmonary resuscitation for refractory cardiac arrest: A multicentre experience. Int J Cardiol. 2017;231:131–136. doi: 10.1016/j.ijcard.2016.12.003. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
