

Echocardiographic Correlates of In-Hospital Death in Patients with Acute COVID-19 Infection: The World Alliance Societies of Echocardiography (WASE-COVID) Study
- PMID: 34023454
- PMCID: PMC8137346
- DOI: 10.1016/j.echo.2021.05.010
Echocardiographic Correlates of In-Hospital Death in Patients with Acute COVID-19 Infection: The World Alliance Societies of Echocardiography (WASE-COVID) Study
Abstract
Background: The novel severe acute respiratory syndrome coronavirus-2 virus, which has led to the global coronavirus disease-2019 (COVID-19) pandemic is known to adversely affect the cardiovascular system through multiple mechanisms. In this international, multicenter study conducted by the World Alliance Societies of Echocardiography, we aim to determine the clinical and echocardiographic phenotype of acute cardiac disease in COVID-19 patients, to explore phenotypic differences in different geographic regions across the world, and to identify parameters associated with in-hospital mortality.
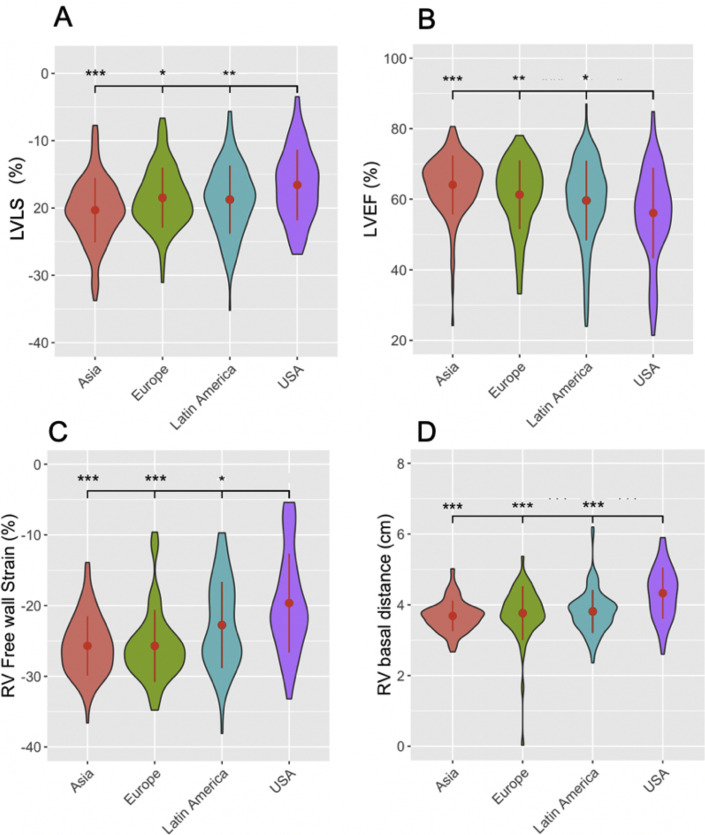
Methods: We studied 870 patients with acute COVID-19 infection from 13 medical centers in four world regions (Asia, Europe, United States, Latin America) who had undergone transthoracic echocardiograms. Clinical and laboratory data were collected, including patient outcomes. Anonymized echocardiograms were analyzed with automated, machine learning-derived algorithms to calculate left ventricular (LV) volumes, ejection fraction, and LV longitudinal strain (LS). Right-sided echocardiographic parameters that were measured included right ventricular (RV) LS, RV free-wall strain (FWS), and RV basal diameter. Multivariate regression analysis was performed to identify clinical and echocardiographic parameters associated with in-hospital mortality.
Results: Significant regional differences were noted in terms of patient comorbidities, severity of illness, clinical biomarkers, and LV and RV echocardiographic metrics. Overall in-hospital mortality was 21.6%. Parameters associated with mortality in a multivariate analysis were age (odds ratio [OR] = 1.12 [1.05, 1.22], P = .003), previous lung disease (OR = 7.32 [1.56, 42.2], P = .015), LVLS (OR = 1.18 [1.05, 1.36], P = .012), lactic dehydrogenase (OR = 6.17 [1.74, 28.7], P = .009), and RVFWS (OR = 1.14 [1.04, 1.26], P = .007).
Conclusions: Left ventricular dysfunction is noted in approximately 20% and RV dysfunction in approximately 30% of patients with acute COVID-19 illness and portend a poor prognosis. Age at presentation, previous lung disease, lactic dehydrogenase, LVLS, and RVFWS were independently associated with in-hospital mortality. Regional differences in cardiac phenotype highlight the significant differences in patient acuity as well as echocardiographic utilization in different parts of the world.
Keywords: COVID-19; Echocardiography; International; Mortality; Strain; WASE.
Copyright © 2021 American Society of Echocardiography. Published by Elsevier Inc. All rights reserved.
Figures




Comment in
-
Timely Identification of Hospitalized Patients at Risk for COVID-19-Associated Right Heart Failure Should Be a Major Goal of Echocardiographic Surveillance.J Am Soc Echocardiogr. 2021 Dec;34(12):1323. doi: 10.1016/j.echo.2021.08.020. Epub 2021 Sep 4. J Am Soc Echocardiogr. 2021. PMID: 34492343 Free PMC article. No abstract available.
-
Response to Letter to the Editor: Timely Identification of Hospitalized Patients at Risk for COVID-19-Associated Right Heart Failure Should Be a Major Goal of Echocardiographic Surveillance.J Am Soc Echocardiogr. 2022 Jun;35(6):669. doi: 10.1016/j.echo.2022.01.014. Epub 2022 Feb 5. J Am Soc Echocardiogr. 2022. PMID: 35134518 Free PMC article. No abstract available.
References
-
- World Health Organization . 2020. Coronavirus disease (COVID-19) pandemic.https://covid19.who.int/ Available at:
-
- Navar A.M. Impact of cardiovascular disease on outcomes among hospitalized COVID-19 patients: results from >14,000 patients across the United States. Virtual AHA Scientific Sessions. 2020 https://www.ahajournals.org/doi/10.1161/CIR.0000000000000940 Available at: - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
