

Re-Irradiation in Patients with Recurrent Rectal Cancer is Safe and Feasible
- PMID: 34023946
- PMCID: PMC8349344
- DOI: 10.1245/s10434-021-10070-6
Re-Irradiation in Patients with Recurrent Rectal Cancer is Safe and Feasible
Abstract
Background: There is no consensus yet for the best treatment regimen in patients with recurrent rectal cancer (RRC). This study aims to evaluate toxicity and oncological outcomes after re-irradiation in patients with RRC in our center. Clinical (cCR) and pathological complete response (pCR) rates and radicality were also studied.
Methods: Between January 2010 and December 2018, 61 locally advanced RRC patients were treated and analyzed retrospectively. Patients received radiotherapy at a dose of 30.0-30.6 Gy (reCRT) or 50.0-50.4 Gy chemoradiotherapy (CRT) in cases of no prior irradiation because of low-risk primary rectal cancer. In both groups, patients received capecitabine concomitantly.
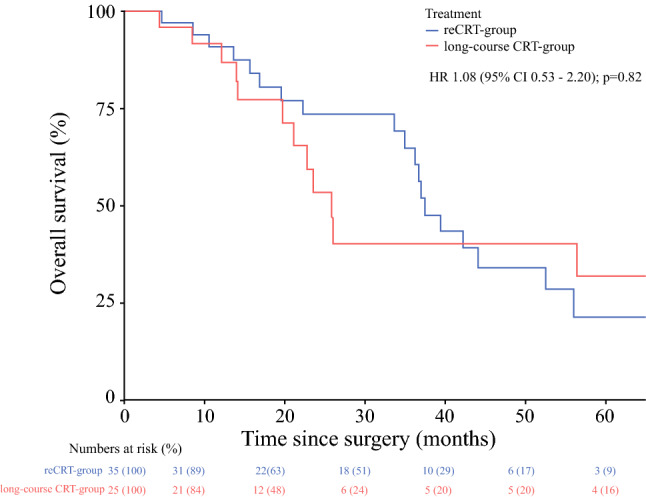
Results: In total, 60 patients received the prescribed neoadjuvant (chemo)radiotherapy followed by surgery, 35 patients (58.3%) in the reRCT group and 25 patients (41.7%) in the long-course CRT group. There were no significant differences in overall survival (p = 0.82), disease-free survival (p = 0.63), and local recurrence-free survival (p = 0.17) between the groups. Patients in the long-course CRT group reported more skin toxicity after radiotherapy (p = 0.040). No differences were observed in late toxicity. In the long-course CRT group, a significantly higher cCR rate was observed (p = 0.029); however, there was no difference in the pCR rate (p = 0.66).
Conclusions: The treatment of RRC patients with re-irradiation is comparable to treatment with long-course CRT regarding toxicity and oncological outcomes. In the reCRT group, less cCR was observed, although there was no difference in pCR. The findings in this study suggest that it is safe and feasible to re-irradiate RRC patients.
© 2021. The Author(s).
Conflict of interest statement
Esmée A. Dijkstra, Véronique E.M. Mul, Patrick H.J. Hemmer, Klaas Havenga, Prof. Geke A.P. Hospers, Christina T. Muijs, and Boudewijn van Etten declare no conflicts of interest, commercial support, financial support, or material support in relation to this manuscript.
Figures


Comment in
-
Chemo-Re-Irradiation and Salvage Surgery for Locally Recurrent Rectal Cancer.Ann Surg Oncol. 2021 Sep;28(9):4769-4771. doi: 10.1245/s10434-021-10198-5. Epub 2021 May 24. Ann Surg Oncol. 2021. PMID: 34031771 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
