

The Mini-Craniotomy for cSDH Revisited: New Perspectives
- PMID: 34025564
- PMCID: PMC8134699
- DOI: 10.3389/fneur.2021.660885
The Mini-Craniotomy for cSDH Revisited: New Perspectives
Abstract
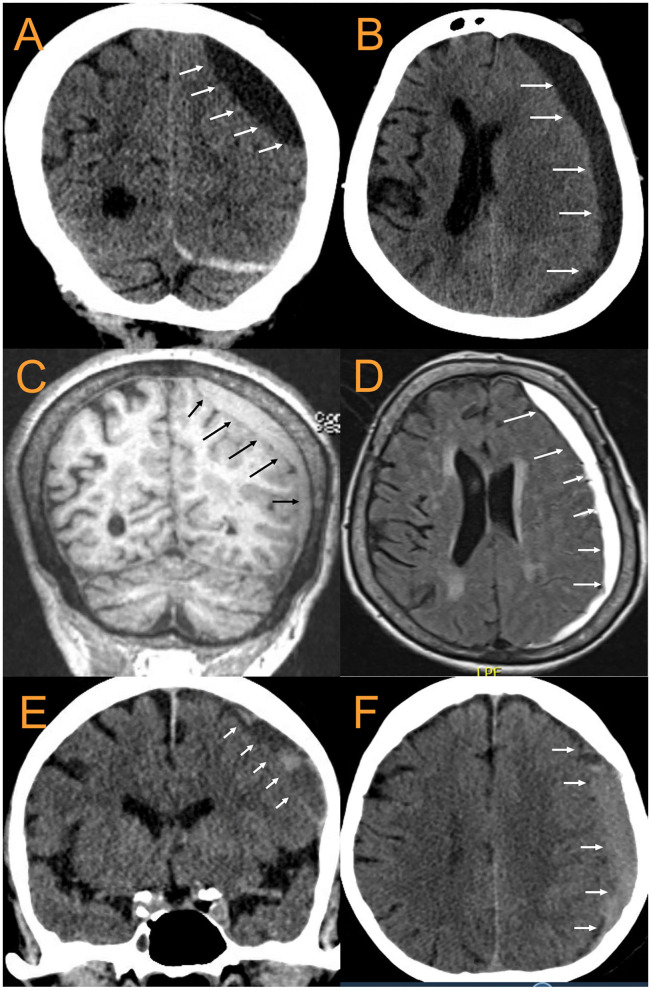
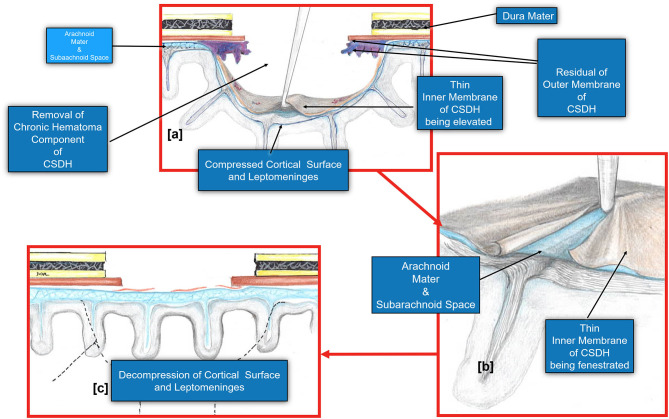
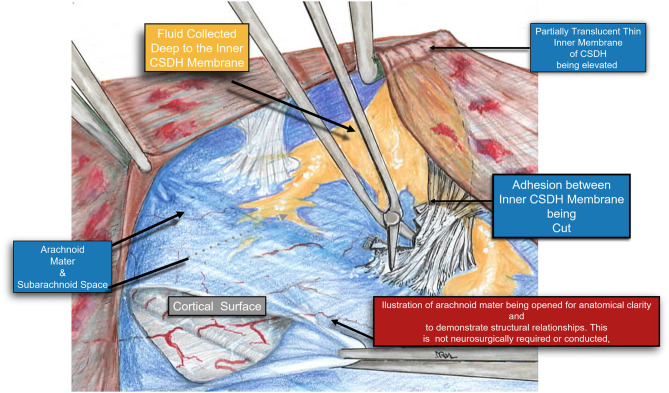
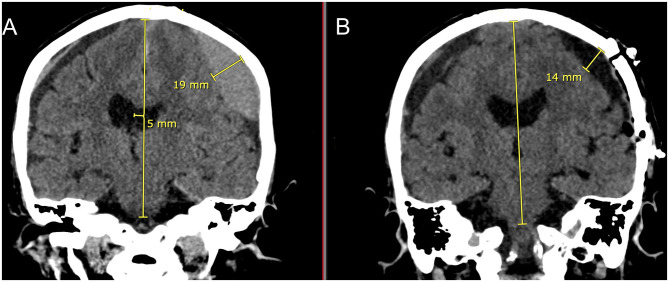
Background: Chronic subdural hematomas (cSDH) are increasingly prevalent worldwide with the increased aging population and anticoagulant use. Different surgical, medical, and endovascular treatments have had varying success rates. Primary neurosurgical interventions include burr hole drainage of the cSDH and mini-craniotomies/craniotomies with or without fenestration of the inner membrane. A key assessment of the success or failure of cSDH treatments has been symptomatic recurrence rates which have historically ranged from 5 to 30%. Pre-operative prediction of the inner subdural membrane by CT scan was used to guide our decision to perform mini-craniotomies. Release of the inner membrane facilitates the expansion of the brain and likely improves glymphatic flow. Methods: Consecutive mini-craniotomies (N = 34) for cSDH evacuation performed by a single neurosurgeon at a quaternary academic medical center/Level I trauma center from July 2018-September 2020 were retrospectively reviewed. Patient characteristics [age, gender, presenting GCS, GOS, initial CTs noting the inner subdural membrane, midline shift (MLS), cSDH width, inner membrane fenestration, cSDH recurrence, post-operative seizures, infections, length of stay] were extracted from the EMR. Results: Twenty nine patients had mini-craniotomies as primary treatment of the cSDH. Mean age = 68.9 ± 19.7 years (range 22-102), mean pre-operative GCS = 14.5 ± 1.1, mean MLS = 6.75 ± 4.2 mm, and mean maximum thickness of cSDH = 17.7 ± 6.0 mm. Twenty four were unilateral, five bilateral, 34 total craniotomies were performed. Thirty three had inner membrane signs on pre-operative head CTs and an inner subdural membrane was fenestrated in all cases except for the one craniotomy that didn't show these characteristic CT findings. Mean operating time = 79.5 ± 26.0 min. Radiographic and clinical improvement occurred in all patients. Mean improvement in MLS = 3.85 ± 2.69. There were no symptomatic recurrences, re-operations, surgical site infections, or deaths during the 6 months of follow-up. One patient was treated for post-operative seizures with AEDs for 6 months. Conclusion: Pre-operative CT scans demonstrating inner subdural membranes may guide one to target the treatment to allow release of this tension band. Mini-craniotomy with careful fenestration of the inner membrane is very effective for this. Brain re-expansion and re-establishment of normal brain interstitial flow may be important in long term outcomes with cSDH and may be related to the recent interests in brain glymphatics and dural lymphatics.
Keywords: chronic subdural hematoma; dural lymphatics; fenestration; glymphatics; inner membrane; mini-craniotomy; neurosurgery.
Copyright © 2021 Chen, Xu, Malkasian, Perez-Rosendahl and Tran.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The subdural evacuation port system: outcomes from a single institution experience and predictors of success.Clin Neurol Neurosurg. 2013 Jun;115(6):658-64. doi: 10.1016/j.clineuro.2012.07.017. Epub 2012 Aug 3. Clin Neurol Neurosurg. 2013. PMID: 22863544
-
Comparative Study of Single Burr-Hole Craniostomy versus Twist-Drill Craniostomy in Patients with Chronic Subdural Hematoma.Asian J Neurosurg. 2019 Apr-Jun;14(2):513-521. doi: 10.4103/ajns.AJNS_37_19. Asian J Neurosurg. 2019. PMID: 31143272 Free PMC article.
-
Use of twist-drill craniostomy with drain in evacuation of chronic subdural hematomas: independent predictors of recurrence.Acta Neurochir (Wien). 2011 May;153(5):1097-103. doi: 10.1007/s00701-010-0903-3. Epub 2010 Dec 31. Acta Neurochir (Wien). 2011. PMID: 21193935
-
Which surgical procedure is effective for refractory chronic subdural hematoma? Analysis of our surgical procedures and literature review.J Clin Neurosci. 2018 Mar;49:40-47. doi: 10.1016/j.jocn.2017.11.009. Epub 2017 Dec 20. J Clin Neurosci. 2018. PMID: 29274740 Review.
-
Chronic subdural hematoma.Asian J Neurosurg. 2016 Oct-Dec;11(4):330-342. doi: 10.4103/1793-5482.145102. Asian J Neurosurg. 2016. PMID: 27695533 Free PMC article. Review.
Cited by
-
The Efficacy of Adjuvant Corticosteroids in Surgical Management of Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis.Front Neurol. 2022 Jan 13;12:744266. doi: 10.3389/fneur.2021.744266. eCollection 2021. Front Neurol. 2022. PMID: 35095713 Free PMC article.
-
Hematoma cavity separation and neomembrane thickness are potential triggers of recurrence of chronic subdural hematoma.BMC Surg. 2022 Jun 20;22(1):236. doi: 10.1186/s12893-022-01687-9. BMC Surg. 2022. PMID: 35725399 Free PMC article.
-
The clinical differences between traumatic and NOS chronic subdural hematoma.Front Neurol. 2024 Oct 17;15:1453629. doi: 10.3389/fneur.2024.1453629. eCollection 2024. Front Neurol. 2024. PMID: 39484047 Free PMC article.
-
Glymphatics for the Neurosurgeon.Neurosurg Pract. 2023 Jul 11;4(3):e00051. doi: 10.1227/neuprac.0000000000000051. eCollection 2023 Sep. Neurosurg Pract. 2023. PMID: 39958788 Free PMC article. Review.
-
The glymphatic system for neurosurgeons: a scoping review.Neurosurg Rev. 2024 Jan 23;47(1):61. doi: 10.1007/s10143-024-02291-6. Neurosurg Rev. 2024. PMID: 38253938 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials