

Early-Warning Immune Predictors for Invasive Pulmonary Aspergillosis in Severe Patients With Severe Fever With Thrombocytopenia Syndrome
- PMID: 34025635
- PMCID: PMC8138034
- DOI: 10.3389/fimmu.2021.576640
Early-Warning Immune Predictors for Invasive Pulmonary Aspergillosis in Severe Patients With Severe Fever With Thrombocytopenia Syndrome
Abstract
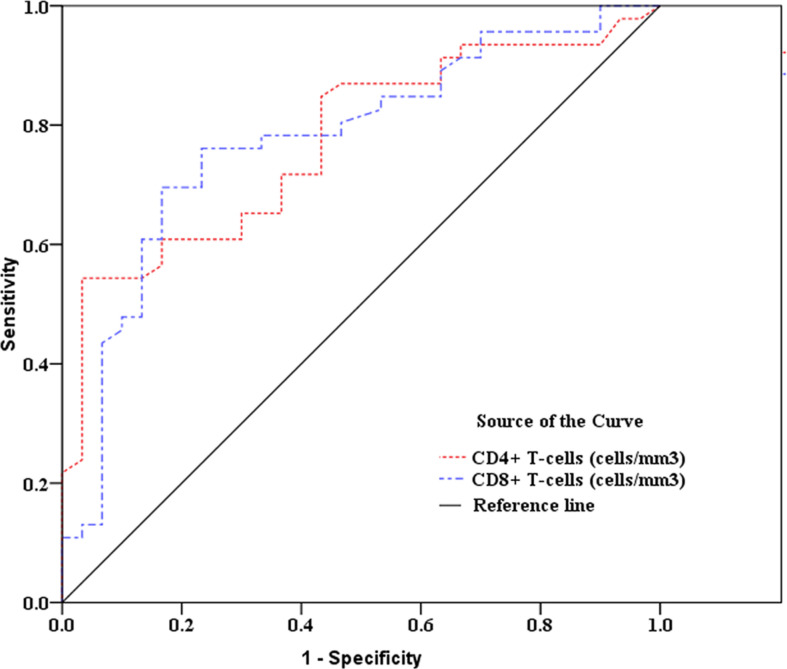
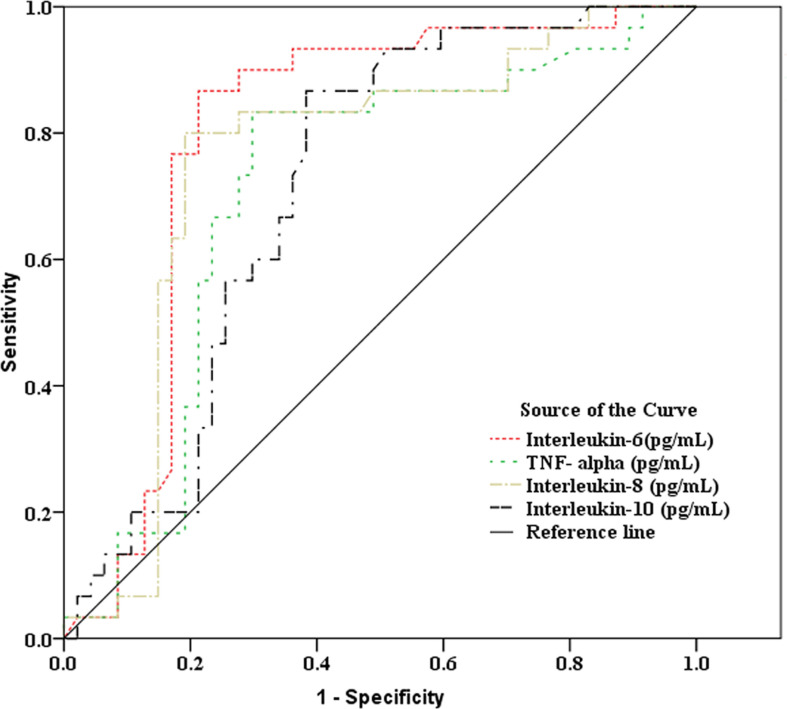
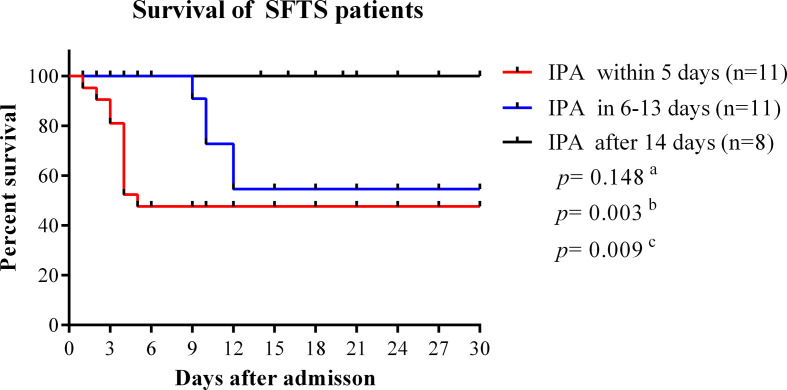
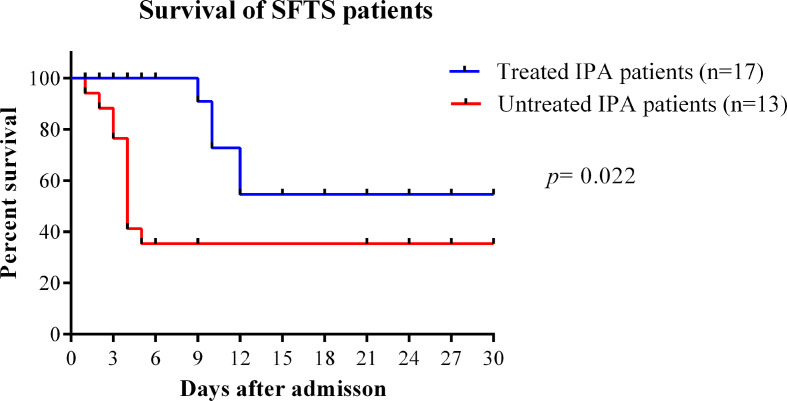
Aspergillus-related disease was confirmed to be associated with immune disorders in patients, severe patients with severe fever with thrombocytopenia syndrome (SFTS) infected by novel phlebovirus were confirmed to have severe immune damage including cellular immunosuppression and cytokine storms. Secondary invasive pulmonary aspergillosis (IPA) in severe SFTS patients can increase fatality rate. This study investigated early-warning predictive factors of secondary IPA in severe SFTS patients. Receiver operating characteristic analysis was used to assess the value of immune parameters to predict IPA in SFTS patients. The cut-off values of CD4+ and CD8+ T-cell counts to predict IPA were 68 and 111 cells/mm3, with sensitivities of 82.6% and 72%, and specificities of 56.7% and 83.3%, respectively. Cut-off values of IL-6, TNF-α, IL-8, and IL-10 to predict IPA incidence in critically ill SFTS patients were 99 pg/mL, 63 pg/mL, 120 pg/mL, and 111 pg/mL, with sensitivities of 90.0%, 86.7%, 83.3% and 90.0% and specificities of 80.4%, 71.7%, 82.6% and 65.2%, respectively. Lower CD4+ and CD8+ T-cells counts, higher levels of IL-6, TNF-α, IL-8 and IL-10, higher incidence of pancreatic and renal damage, early antibacterial therapy of carbapenems, and intensive care unit admission were risk factors of IPA in SFTS patients. Multivariate logistic regression analysis indicated counts of CD4+ T-cells <68 cells/mm3 combined with CD8+ T-cells <111 cells/mm3 (odds ratio [OR] 0.218, 95% confidence interval [CI] 0.059-0.803, p=0.022), IL-6 >99 pg/ml combined with IL-10 >111 pg/ml (OR 17.614, 95% CI 2.319-133.769, p=0.006), and brain natriuretic peptide level >500 pg/ml (OR 13.681, 95% CI 1.994-93.871, p=0.008) were independent risk factors for IPA in SFTS patients. The mortality in the IPA group was significantly higher than in the non-IPA group (p=0.001). Early antifungal treatment of IPA patients was significantly associated with improved survival (log-rank, p=0.022). Early diagnosis of IPA and antifungal treatment can improve the prognosis of SFTS patients. Besides, we speculate SFTS may be as a host factor for IPA.
Keywords: immunity; invasive pulmonary aspergillosis; novel phlebovirus; risk factors; severe fever with thrombocytopenia syndrome.
Copyright © 2021 Hu, Kong, Yue, Xu, Xia, Bian, Liu, Zhang, Ma, Yin, Sun, Gao, Ye and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Investigation of predictors for invasive pulmonary aspergillosis in patients with severe fever with thrombocytopenia syndrome.Sci Rep. 2023 Jan 27;13(1):1538. doi: 10.1038/s41598-023-28851-2. Sci Rep. 2023. PMID: 36707667 Free PMC article.
-
Clinical features of fatal severe fever with thrombocytopenia syndrome that is complicated by invasive pulmonary aspergillosis.J Infect Chemother. 2018 Jun;24(6):422-427. doi: 10.1016/j.jiac.2018.01.005. Epub 2018 Feb 7. J Infect Chemother. 2018. PMID: 29428567
-
Cytokines and lymphocyte subsets are associated with disease severity of severe fever with thrombocytopenia syndrome.Virol J. 2024 Jun 3;21(1):126. doi: 10.1186/s12985-024-02403-0. Virol J. 2024. PMID: 38831352 Free PMC article.
-
Severe fever with thrombocytopenia syndrome: a systematic review and meta-analysis of epidemiology, clinical signs, routine laboratory diagnosis, risk factors, and outcomes.BMC Infect Dis. 2020 Aug 5;20(1):575. doi: 10.1186/s12879-020-05303-0. BMC Infect Dis. 2020. PMID: 32758175 Free PMC article.
-
Serial analysis of cytokine and chemokine profiles and viral load in severe fever with thrombocytopenia syndrome: Case report and review of literature.Medicine (Baltimore). 2019 Oct;98(42):e17571. doi: 10.1097/MD.0000000000017571. Medicine (Baltimore). 2019. PMID: 31626125 Free PMC article. Review.
Cited by
-
The pathogenic and clinical characteristics of severe fever with thrombocytopenia syndrome patients with co-infections.Front Cell Infect Microbiol. 2023 Dec 1;13:1298050. doi: 10.3389/fcimb.2023.1298050. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 38106473 Free PMC article.
-
Overview of the immunological mechanism underlying severe fever with thrombocytopenia syndrome (Review).Int J Mol Med. 2022 Sep;50(3):118. doi: 10.3892/ijmm.2022.5174. Epub 2022 Jul 20. Int J Mol Med. 2022. PMID: 35856413 Free PMC article. Review.
-
Cytokine and Chemokine Profiles in Acute Severe Fever with Thrombocytopenia Syndrome and Scrub Typhus in South Korea.Am J Trop Med Hyg. 2023 Oct 30;109(6):1311-1318. doi: 10.4269/ajtmh.23-0146. Print 2023 Dec 6. Am J Trop Med Hyg. 2023. PMID: 37903435 Free PMC article.
-
Longitudinal analysis of cytokine dynamics in severe fever with thrombocytopenia syndrome patients - High-incidence regions of China (2010-2023).Biosaf Health. 2025 Mar 26;7(2):83-93. doi: 10.1016/j.bsheal.2025.03.005. eCollection 2025 Apr. Biosaf Health. 2025. PMID: 40453472 Free PMC article.
-
NLR, A Convenient Early-Warning Biomarker of Fatal Outcome in Patients With Severe Fever With Thrombocytopenia Syndrome.Front Microbiol. 2022 Jun 23;13:907888. doi: 10.3389/fmicb.2022.907888. eCollection 2022. Front Microbiol. 2022. PMID: 35814714 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials