

Anti-N-methyl-d-aspartate receptor encephalitis: A primer for acute care healthcare professionals
- PMID: 34025748
- PMCID: PMC8120570
- DOI: 10.1177/1751143720914181
Anti-N-methyl-d-aspartate receptor encephalitis: A primer for acute care healthcare professionals
Abstract
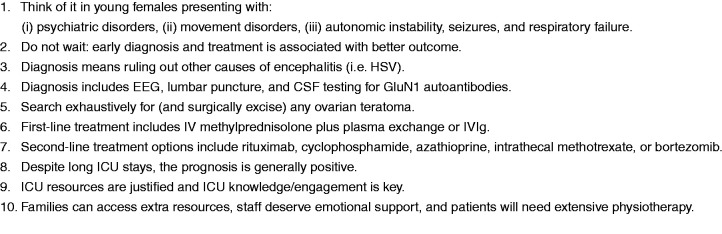
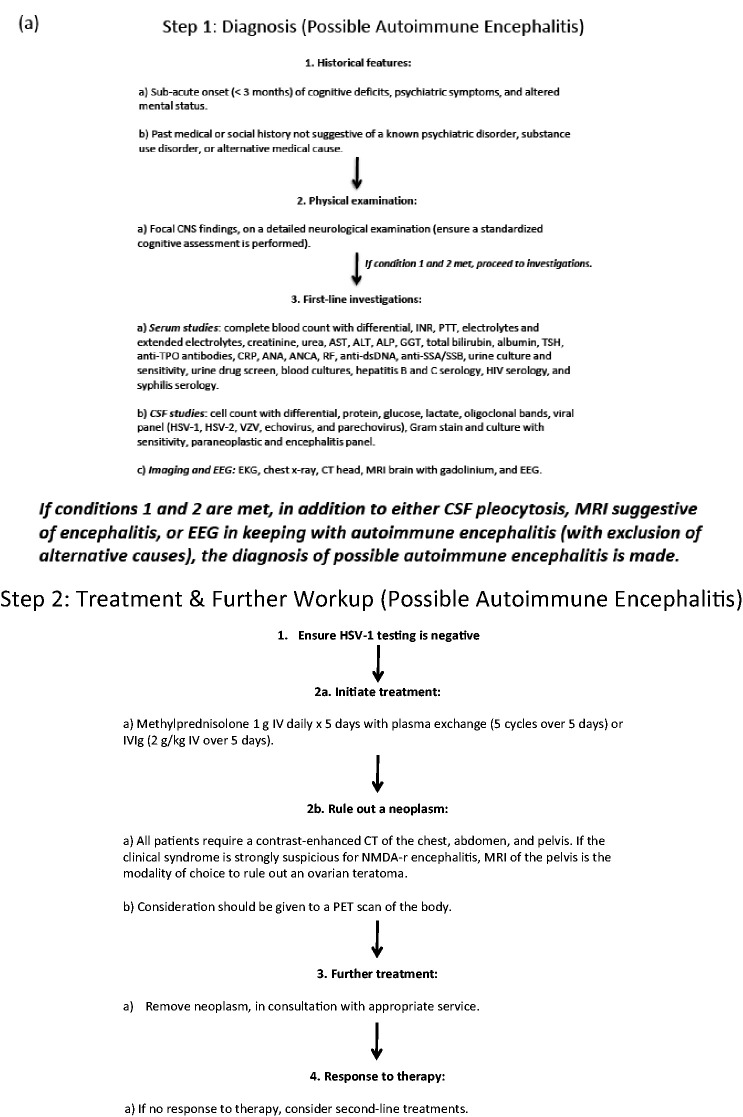
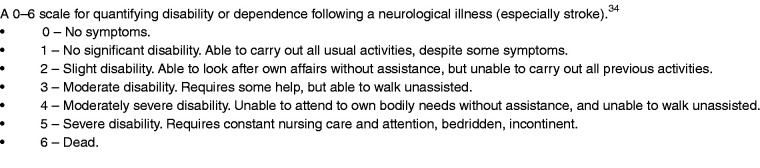
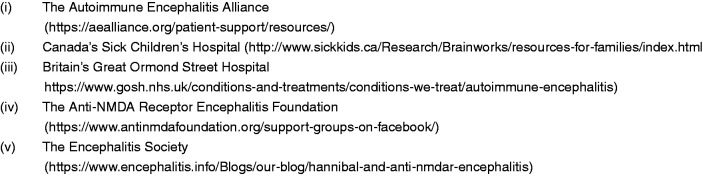
This primer summarizes the diagnosis, treatment, complications, and prognosis of anti-N-methyl-d-aspartate receptor encephalitis for healthcare professionals, especially those in acute care specialities. Anti-N-methyl-d-aspartate receptor encephalitis is an immune-mediated encephalitis that is classically paraneoplastic and associated with ovarian teratomas in young women. Other less common neoplastic triggers include testicular cancers, Hodgkin lymphoma, lung and breast cancers. It may also be triggered by infection, occurring as a para-infectious phenomenon, seen most commonly after herpes simplex-1 encephalitis. Presentation varies but typically consists of behavioural and cognitive manifestations, seizures, dysautonomia, movement disorders, central hypoventilation, and coma, necessitating intensive care unit admission. Diagnosis of anti-N-methyl-d-aspartate receptor encephalitis requires high clinical suspicion plus ancillary testing, the most sensitive being cerebrospinal fluid analysis for anti-N-methyl-d-aspartate receptor antibodies. Imaging in search of an ovarian teratoma should be exhaustive and tumours need to be surgically treated. Treatment should be expeditious with pulsed steroids and either plasma exchange or intravenous immunoglobulin. Second-line treatments include intravenous rituximab, cyclophosphamide, azathioprine, and intrathecal methotrexate. Most patients recover to be functionally independent, but the in-hospital course can be months long followed by extensive rehabilitation. Given the lengthy course of illness, we explain why education and debriefing are important for staff, and where families can obtain additional help.
Keywords: Anti-N-methyl-d-aspartate receptor encephalitis; encephalitis; intensive care unit; ovarian teratoma.
© The Intensive Care Society 2020.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- de Montmollin E, Demeret S, Brule N, et al. Anti-N-methyl-D-aspartate receptor encephalitis in adult patients requiring intensive care. Am J Respir Crit Care Med 2017; 195: 491–499. - PubMed
-
- Mittal MK, Rabinstein AA, Hocker SE, et al. Autoimmune encephalitis in the ICU: analysis of phenotypes, serologic findings, and outcomes. Neurocrit Care 2016; 24: 240–250. - PubMed
LinkOut - more resources
Full Text Sources