

Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Retrosigmoid Approach
- PMID: 34026408
- PMCID: PMC8133810
- DOI: 10.1055/s-0039-1700513
Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Retrosigmoid Approach
Abstract
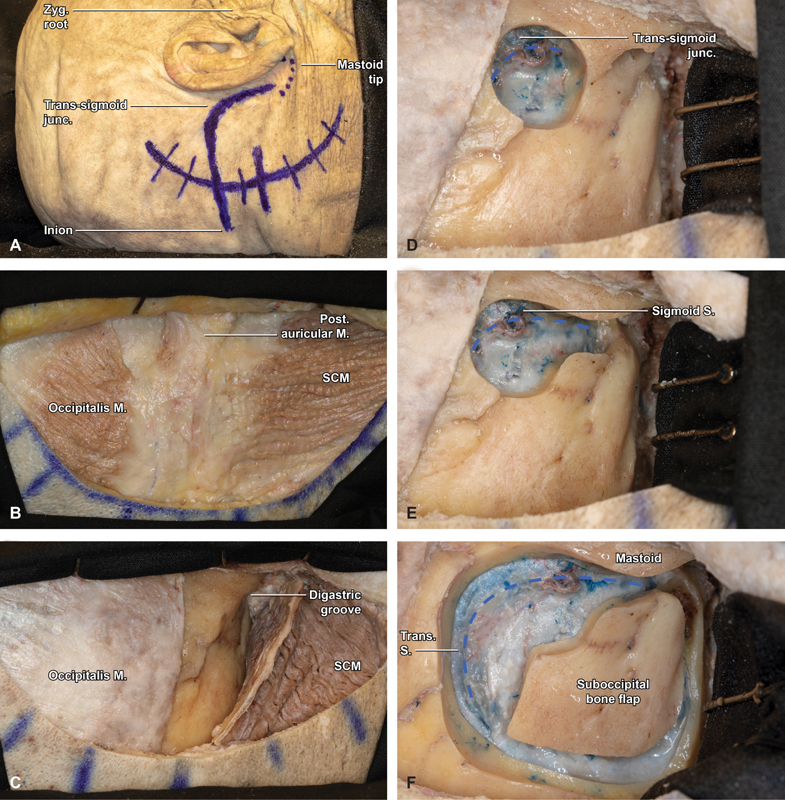
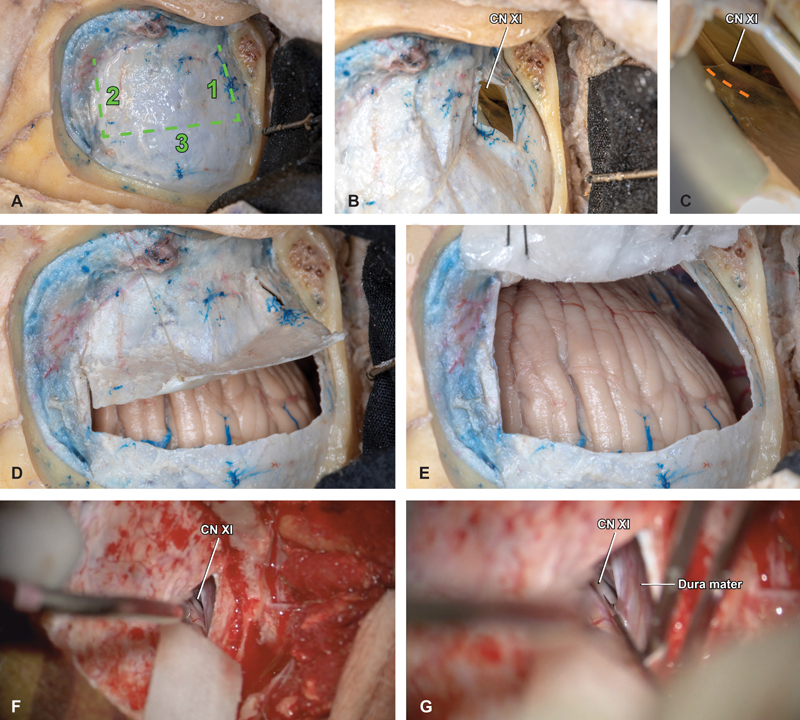
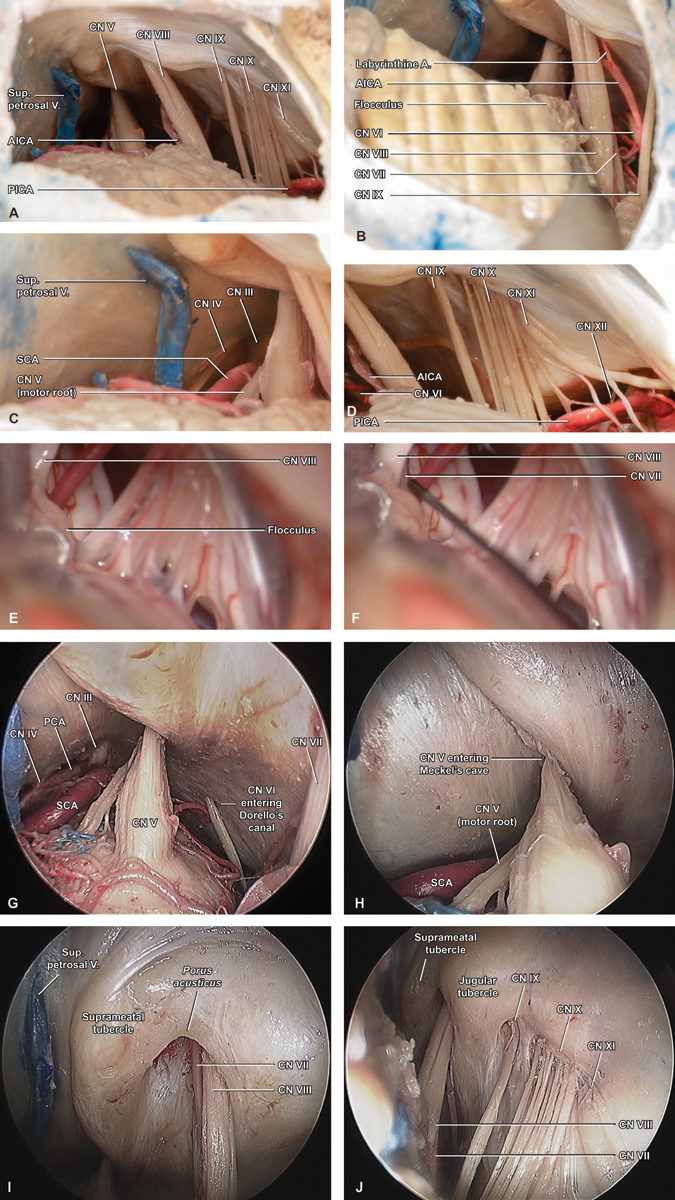
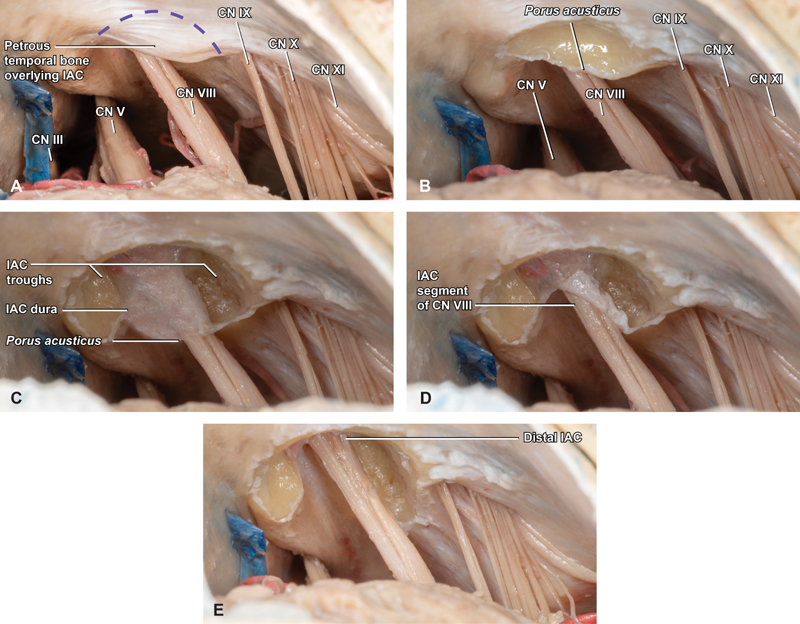
Introduction Neurosurgical anatomy is traditionally taught via anatomic and operative atlases; however, these resources present the skull base using views that emphasize three-dimensional (3D) relationships rather than operative perspectives, and are frequently written above a typical resident's understanding. Our objective is to describe, step-by-step, a retrosigmoid approach dissection, in a way that is educationally valuable for trainees at numerous levels. Methods Six sides of three formalin-fixed latex-injected specimens were dissected under microscopic magnification. A retrosigmoid was performed by each of three neurosurgery residents, under supervision by the senior authors (C.L.W.D. and M.J.L.) and a graduated skull base fellow, neurosurgeon, and neuroanatomist (M.P.C.). Dissections were supplemented with representative case applications. Results The retrosigmoid craniotomy (aka lateral suboccipital approach) affords excellent access to cranial nerve (CN) IV to XII, with corresponding applicability to numerous posterior fossa operations. Key steps include positioning and skin incision, scalp and muscle flaps, burr hole and parasigmoid trough, craniotomy flap elevation, initial durotomy and deep cistern access, completion durotomy, and final exposure. Conclusion The retrosigmoid craniotomy is a workhorse skull base exposure, particularly for lesions located predominantly in the cerebellopontine angle. Operatively oriented neuroanatomy dissections provide trainees with a critical foundation for learning this fundamental skull base technique. We outline a comprehensive approach for neurosurgery residents to develop their familiarity with the retrosigmoid craniotomy in the cadaver laboratory in a way that simultaneously informs rapid learning in the operating room, and an understanding of its potential for wide clinical application to skull base diseases.
Keywords: acoustic neuroma; education; meningioma; retrosigmoid; simulation; skull base; vestibular schwannoma.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest None declared.
Figures
References
-
- Meyer F B. Philadelphia, PA: Churchill Livingstone; 1999. Atlas of Neurosurgery: Basic Approaches to Cranial and Vascular Procedures.
-
- Tew J M, Van Loveren H Keller JT. Philadelphia, PA: Saunders; 1994. Atlas of Operative Microneurosurgery.
-
- Rhoton A L., JrThe cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach Neurosurgery 200047(3, Suppl):S93–S129. - PubMed
-
- Wanibuchi M, Friedman A H, Fukushima T. Stuttgart, Germany: Thieme; 2009. Photo Atlas of Skull Base Dissection: Techniques and Operative Approaches.
