

Internet-Based Cognitive Behavioral Therapy for Patients Reporting Symptoms of Anxiety and Depression After Myocardial Infarction: U-CARE Heart Randomized Controlled Trial Twelve-Month Follow-up
- PMID: 34028358
- PMCID: PMC8185614
- DOI: 10.2196/25465
Internet-Based Cognitive Behavioral Therapy for Patients Reporting Symptoms of Anxiety and Depression After Myocardial Infarction: U-CARE Heart Randomized Controlled Trial Twelve-Month Follow-up
Abstract
Background: The U-CARE Heart trial was one of the first randomized controlled trials to evaluate the effect of internet-based cognitive behavioral therapy on self-reported symptoms of anxiety or depression for patients with a recent myocardial infarction. While the effects of internet-based cognitive behavioral therapy on Hospital Anxiety and Depression Scale (HADS) scores at 14 weeks postbaseline were not significant, in this study, we investigated possible long-term effects of treatment.
Objective: The aim of this study was to evaluate the long-term effectiveness of internet-based cognitive behavioral therapy on self-reported symptoms of anxiety and depression in patients 12 months after a myocardial infarction and to explore subsequent occurrences of cardiovascular disease events.
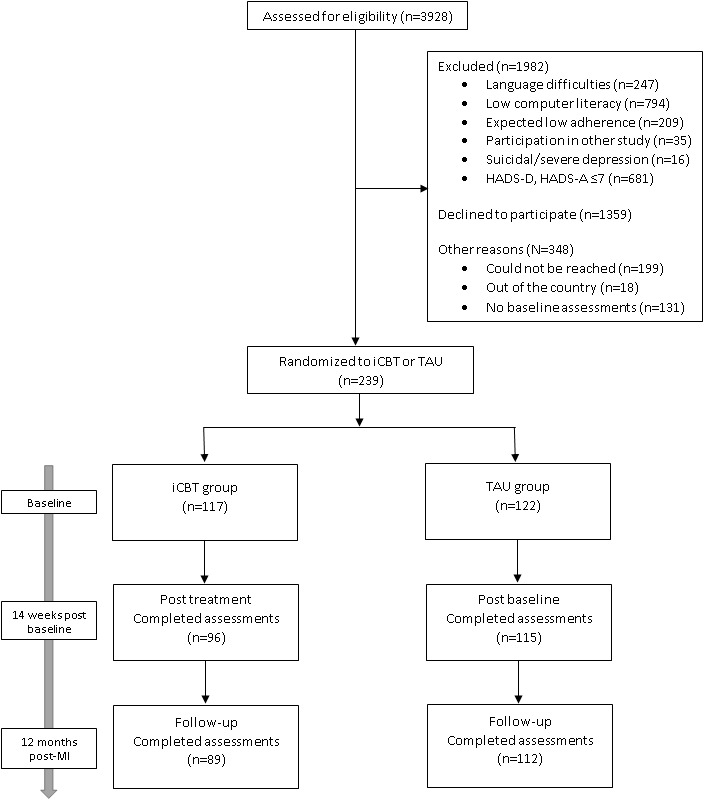
Methods: Shortly after acute myocardial infarction, 239 patients (33% female, mean age 59.6 years) reporting mild-to-moderate symptoms of anxiety or depression were randomized to 14 weeks of therapist-guided internet-based cognitive behavioral therapy (n=117) or treatment as usual (n=122). Data from national registries were used to explore group differences in clinical outcomes such as cardiovascular disease and cardiovascular-related mortality for a follow-up period of up to 5 years: group differences in HADS total score 1 year post-myocardial infarction, the primary outcome, was analyzed using multiple linear regression. Secondary outcomes, such as HADS anxiety and depression subscales and the Cardiac Anxiety Questionnaire total score (CAQ), which measures heart-focused anxiety, were analyzed in the same way. Multiple imputation was used to account for missing data, and a pooled treatment effect was estimated. Adjusted Cox proportional hazards models were used to estimate hazard ratios (HRs) for data pertaining to registry outcomes.
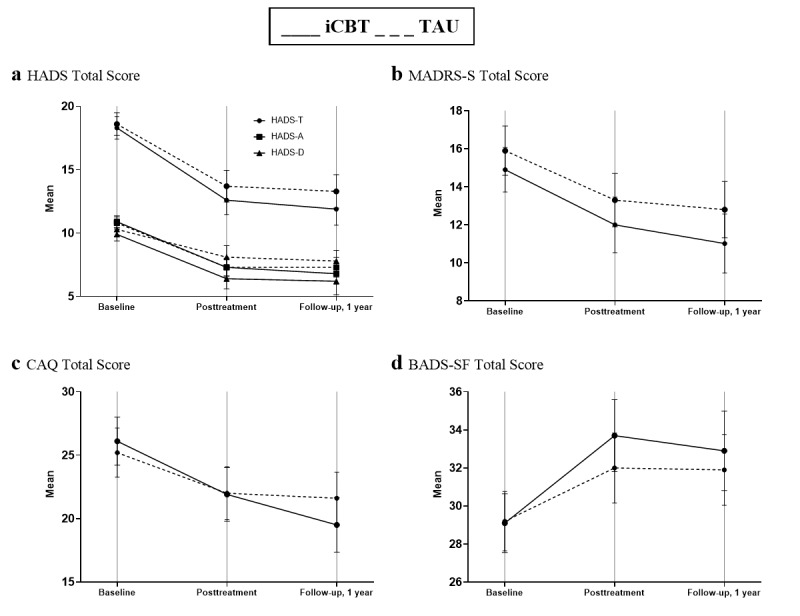
Results: Both groups reported lower HADS total scores 1 year after myocardial infarction than those at baseline. HADS total scores were not significantly different between the treatment and control groups 1 year after myocardial infarction (β=-1.14, 95% CI -2.73 to 0.45, P=.16). CAQ was the only measure improved significantly by internet-based cognitive behavioral therapy when compared with treatment as usual (β=-2.58, 95% CI -4.75 to -0.42, P=.02) before adjusting for multiple comparisons. The composite outcome of nonfatal cardiovascular events and cardiovascular-related mortality did not differ between groups but was numerically higher in the internet-based cognitive behavioral therapy group, who were at slightly greater risk (HR 1.8, 95% CI 0.96 to 3.4, P=.07). Adjusting for previous myocardial infarction and diabetes attenuated this estimate (HR 1.5, 95% CI 0.8 to 2.8, P=.25).
Conclusions: Internet-based cognitive behavioral therapy was not superior in reducing self-reported symptoms of depression or anxiety compared to treatment as usual at the 1-year follow-up after myocardial infarction. A reduction in cardiac-related anxiety was observed but was not significant after adjusting for multiple comparisons. There was no difference in risk of cardiovascular events between the treatment groups. Low treatment adherence, which might have affected treatment engagement and outcomes, should be considered when interpreting these results.
Trial registration: ClinicalTrials.gov NCT01504191; https://clinicaltrials.gov/ct2/show/NCT01504191.
International registered report identifier (irrid): RR2-10.1186/s13063-015-0689-y.
Keywords: anxiety; cardiovascular; cardiovascular health; cognitive behavior therapy; depression; iCBT; infarction; internet; myocardial infarction; psychological treatment; treatment.
©Sophia Monica Humphries, John Wallert, Fredrika Norlund, Emma Wallin, Gunilla Burell, Louise von Essen, Claes Held, Erik Martin Gustaf Olsson. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 24.05.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- GBD 2017 Risk Factor Collaborators Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018 Nov 10;392(10159):1923–1994. doi: 10.1016/S0140-6736(18)32225-6. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(18)32225-6 - DOI - PMC - PubMed
-
- Yusuf S, Hawken S, Ounpuu Stephanie, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L, INTERHEART Study Investigators Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–52. doi: 10.1016/S0140-6736(04)17018-9. - DOI - PubMed
-
- Geiser F, Urbach AS, Harbrecht U, Conrad R, Pötzsch Bernd, Amann N, Kiesewetter K, Sieke A, Wolffs K, Skowasch D. Anxiety and depression in patients three months after myocardial infarction: association with markers of coagulation and the relevance of age. J Psychosom Res. 2017 Aug;99:162–168. doi: 10.1016/j.jpsychores.2017.06.015. - DOI - PubMed
-
- Norlund F, Lissåker Claudia, Wallert J, Held C, Olsson EM. Factors associated with emotional distress in patients with myocardial infarction: results from the SWEDEHEART registry. Eur J Prev Cardiol. 2018 Jun;25(9):910–920. doi: 10.1177/2047487318770510. https://tinyurl.com/k5vn6ssz - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
