

Delivery Room Interventions for Hypothermia in Preterm Neonates: A Systematic Review and Network Meta-analysis
- PMID: 34028513
- PMCID: PMC8145154
- DOI: 10.1001/jamapediatrics.2021.0775
Delivery Room Interventions for Hypothermia in Preterm Neonates: A Systematic Review and Network Meta-analysis
Abstract
Importance: Prevention of hypothermia in the delivery room is a cost-effective, high-impact intervention to reduce neonatal mortality, especially in preterm neonates. Several interventions for preventing hypothermia in the delivery room exist, of which the most beneficial is currently unknown.
Objective: To identify the delivery room thermal care intervention that can best reduce neonatal hypothermia and improve clinical outcomes for preterm neonates born at 36 weeks' gestation or less.
Data sources: MEDLINE, the Cochrane Central Register of Controlled Trials, Embase, and CINAHL databases were searched from inception to November 5, 2020.
Study selection: Randomized and quasi-randomized clinical trials of thermal care interventions in the delivery room for preterm neonates were included. Peer-reviewed abstracts and studies published in non-English language were also included.
Data extraction and synthesis: Data from the included trials were extracted in duplicate using a structured proforma. A network meta-analysis with bayesian random-effects model was used for data synthesis.
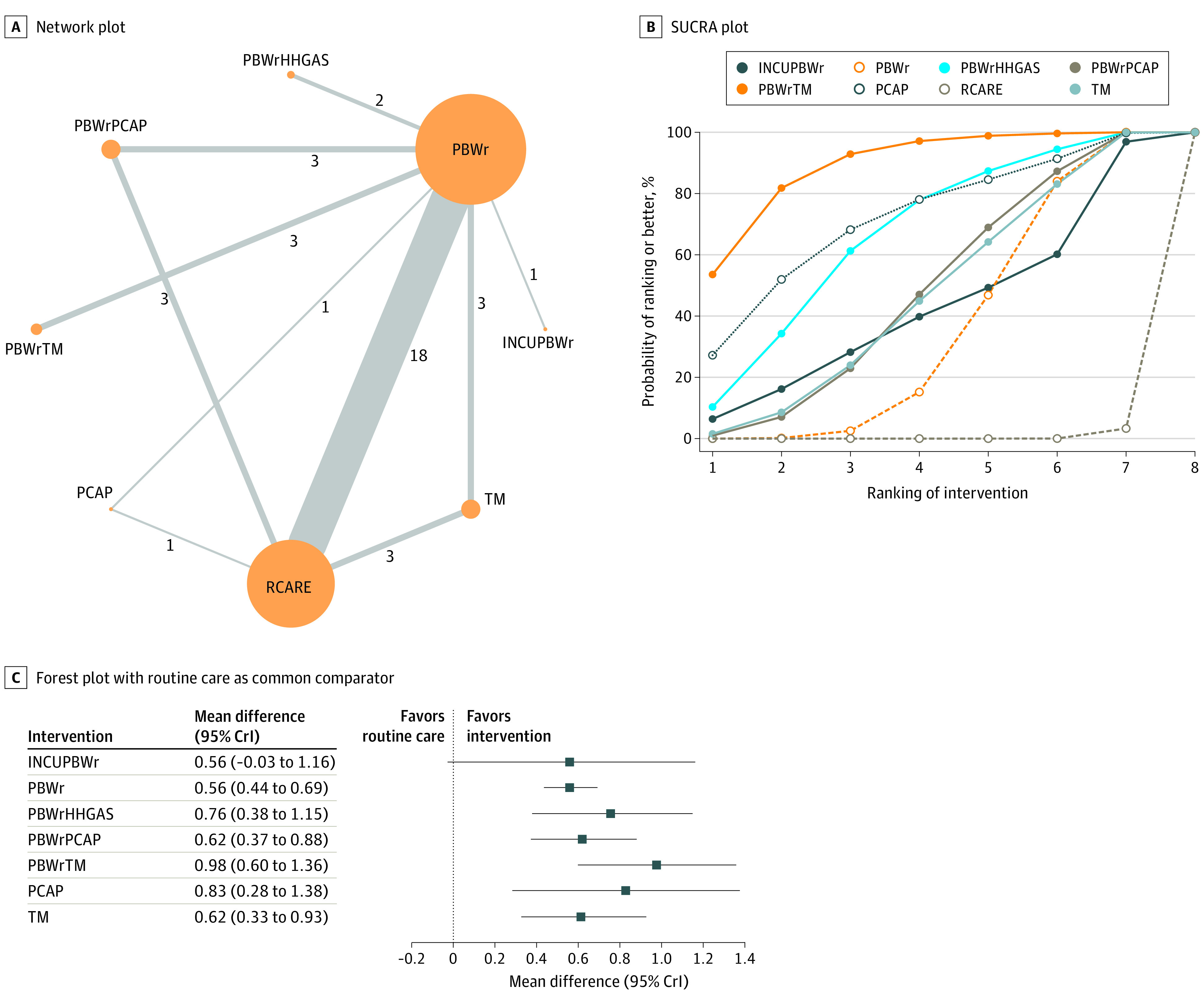
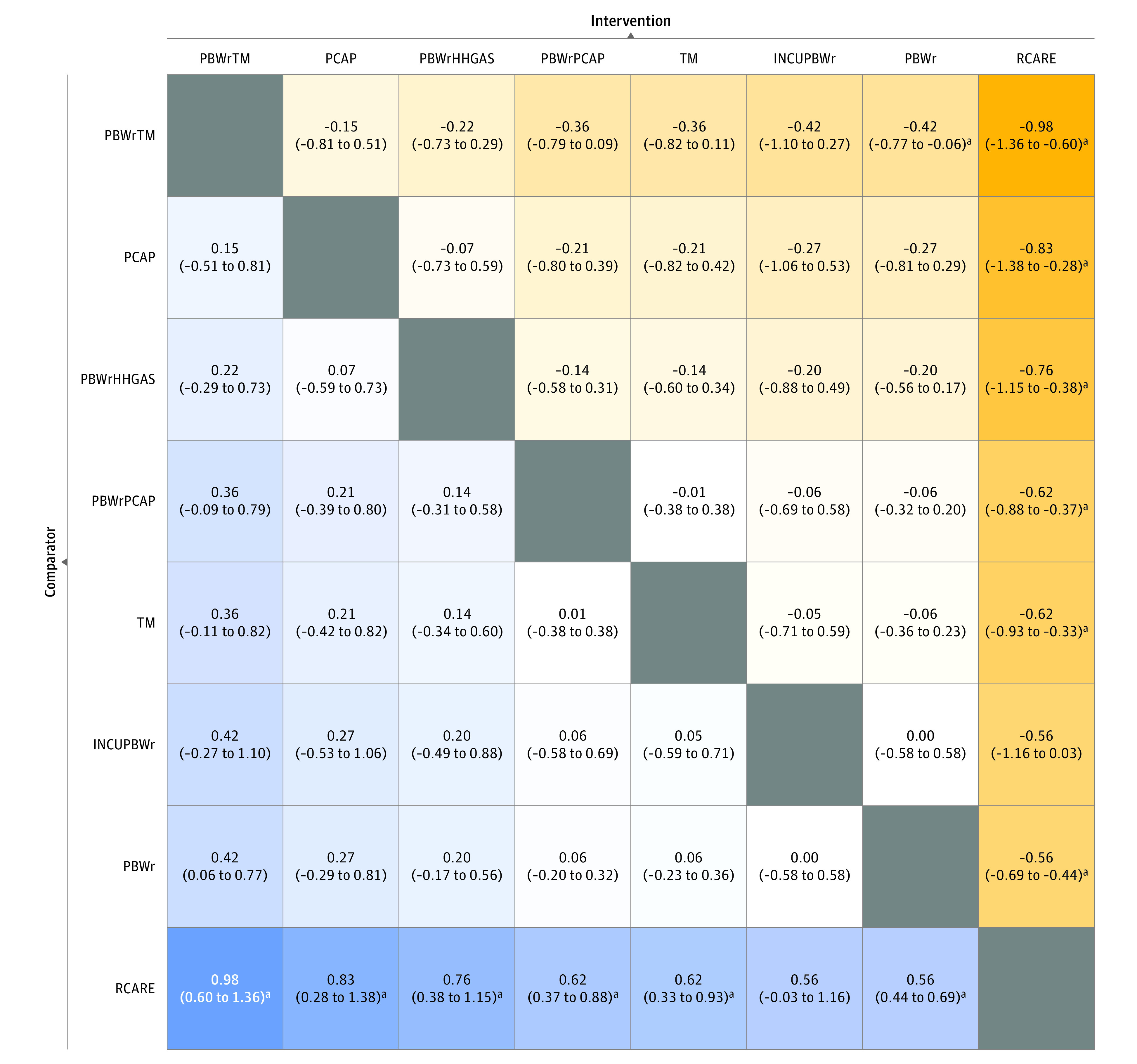
Main outcomes and measures: Primary outcomes were core body temperature and incidence of moderate to severe hypothermia on admission or within the first 2 hours of life. Secondary outcomes were incidence of hyperthermia, major brain injury, and mortality before discharge. The 9 thermal interventions evaluated were (1) plastic bag or plastic wrap covering the torso and limbs with the head uncovered or covered with a cloth cap; (2) plastic cap covering the head; (3) skin-to-skin contact; (4) thermal mattress; (5) plastic bag or plastic wrap with a plastic cap; (6) plastic bag or plastic wrap along with use of a thermal mattress; (7) plastic bag or plastic wrap along with heated humidified gas for resuscitation or for initiating respiratory support in the delivery room; (8) plastic bag or plastic wrap along with an incubator for transporting from the delivery room; and (9) routine care, including drying and covering the body with warm blankets, with or without a cloth cap.
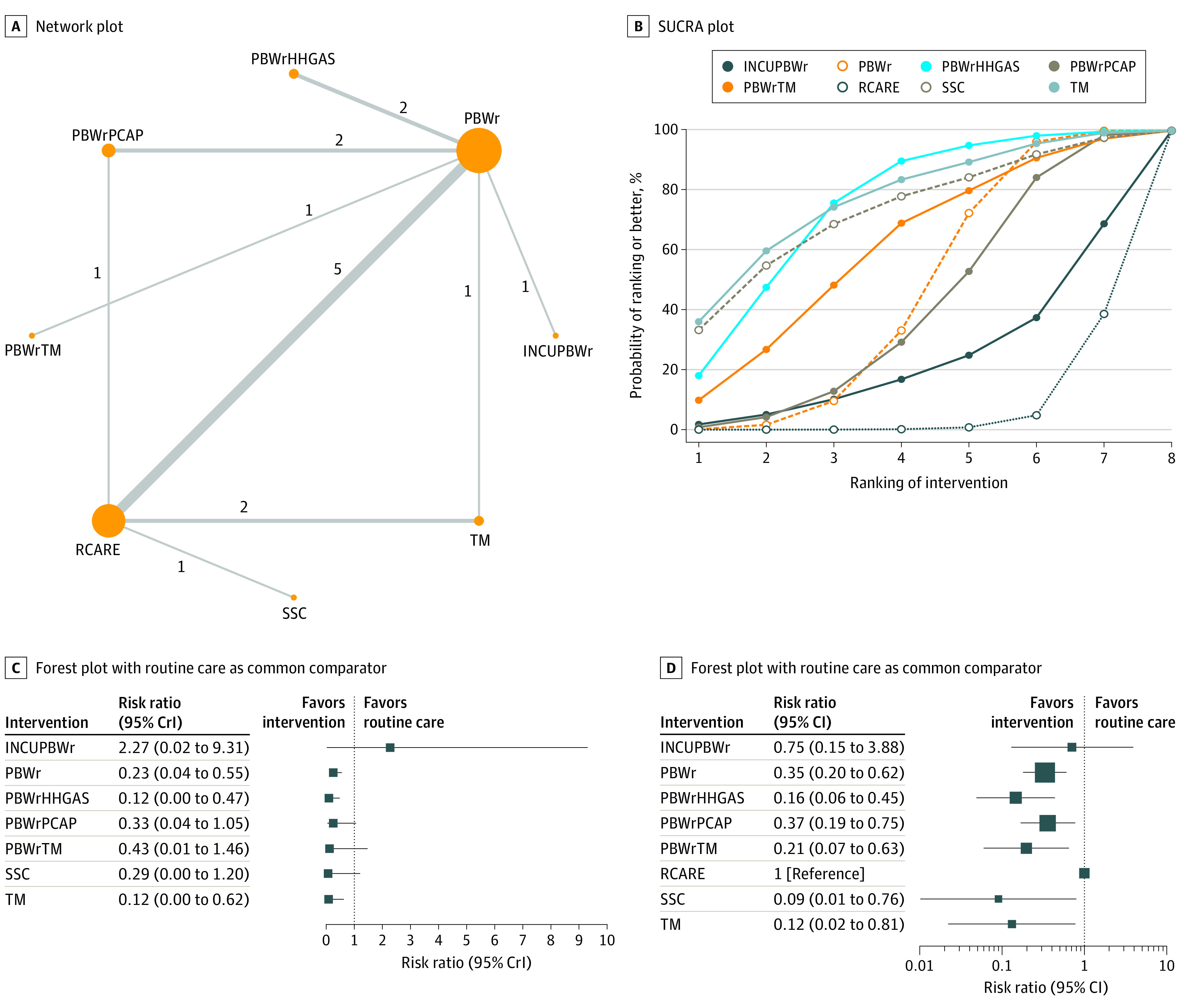
Results: Of the 6154 titles and abstracts screened, 34 studies that enrolled 3688 neonates were analyzed. Compared with routine care alone, plastic bag or wrap with a thermal mattress (mean difference [MD], 0.98 °C; 95% credible interval [CrI], 0.60-1.36 °C), plastic cap (MD, 0.83 °C; 95% CrI, 0.28-1.38 °C), plastic bag or wrap with heated humidified respiratory gas (MD, 0.76 °C; 95% CrI, 0.38-1.15 °C), plastic bag or wrap with a plastic cap (MD, 0.62 °C; 95% CrI, 0.37-0.88 °C), thermal mattress (MD, 0.62 °C; 95% CrI, 0.33-0.93 °C), and plastic bag or wrap (MD, 0.56 °C; 95% CrI, 0.44-0.69 °C) were associated with greater core body temperature. Certainty of evidence was moderate for 5 interventions and low for plastic bag or wrap with a thermal mattress. When compared with routine care alone, a plastic bag or wrap with heated humidified respiratory gas was associated with less risk of major brain injury (risk ratio, 0.23; 95% CrI, 0.03-0.67; moderate certainty of evidence) and a plastic bag or wrap with a plastic cap was associated with decreased risk of mortality (risk ratio, 0.19; 95% CrI, 0.02-0.66; low certainty of evidence).
Conclusions and relevance: Results of this study indicate that most thermal care interventions in the delivery room for preterm neonates were associated with improved core body temperature (with moderate certainty of evidence). Specifically, use of a plastic bag or wrap with a plastic cap or with heated humidified gas was associated with lower risk of major brain injury and mortality (with low to moderate certainty of evidence).
Conflict of interest statement
Figures
Comment in
-
Delivery room thermal care interventions in preterm neonates.Acta Paediatr. 2022 Jan;111(1):196-197. doi: 10.1111/apa.16092. Epub 2021 Sep 16. Acta Paediatr. 2022. PMID: 34532887 No abstract available.
References
-
- Vermont Oxford Network . Despite decreases, nearly 4 in 10 infants are cold when admitted to the NICU. Accessed December 5, 2020. https://public.vtoxford.org/nicu-by-the-numbers/despite-decreases-nearly...
-
- Laptook AR, Bell EF, Shankaran S, et al. ; Generic and Moderate Preterm Subcommittees of the NICHD Neonatal Research Network . Admission temperature and associated mortality and morbidity among moderately and extremely preterm infants. J Pediatr. 2018;192:53-59.e2. doi:10.1016/j.jpeds.2017.09.021 - DOI - PMC - PubMed
-
- de Siqueira Caldas JP, Ferri WAG, Marba STM, et al. . Admission hypothermia, neonatal morbidity, and mortality: evaluation of a multicenter cohort of very low birth weight preterm infants according to relative performance of the center. Eur J Pediatr. 2019;178(7):1023-1032. doi:10.1007/s00431-019-03386-9 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
