

NGAL/hepcidin-25 ratio and AKI subtypes in patients following cardiac surgery: a prospective observational study
- PMID: 34028701
- PMCID: PMC8926978
- DOI: 10.1007/s40620-021-01063-5
NGAL/hepcidin-25 ratio and AKI subtypes in patients following cardiac surgery: a prospective observational study
Abstract
Background: Acute kidney injury (AKI) subtypes combining kidney functional parameters and injury biomarkers may have prognostic value. We aimed to determine whether neutrophil gelatinase-associated lipocalin (NGAL)/hepcidin-25 ratio (urinary concentrations of NGAL divided by that of hepcidin-25) defined subtypes are of prognostic relevance in cardiac surgery patients.
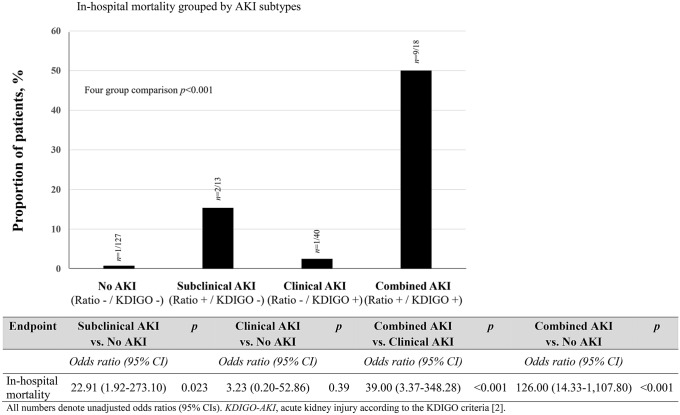
Methods: We studied 198 higher-risk cardiac surgery patients. We allocated patients to four groups: Kidney Disease Improving Global Outcomes (KDIGO)-AKI-negative and NGAL/hepcidin-25 ratio-negative (no AKI), KDIGO AKI-negative and NGAL/hepcidin-25 ratio-positive (subclinical AKI), KDIGO AKI-positive and NGAL/hepcidin-25 ratio-negative (clinical AKI), KDIGO AKI-positive and NGAL/hepcidin-25 ratio-positive (combined AKI). Outcomes included in-hospital mortality (primary) and long-term mortality (secondary).
Results: We identified 127 (61.6%) patients with no AKI, 13 (6.6%) with subclinical, 40 (20.2%) with clinical and 18 (9.1%) with combined AKI. Subclinical AKI patients had a 23-fold greater in-hospital mortality than no AKI patients. For combined AKI vs. no AKI or clinical AKI, findings were stronger (odds ratios (ORs): 126 and 39, respectively). After adjusting for EuroScore, volume of intraoperative packed red blood cells, and aortic cross-clamp time, subclinical and combined AKI remained associated with greater in-hospital mortality than no AKI and clinical AKI (adjusted ORs: 28.118, 95% CI 1.465-539.703; 3.737, 95% CI 1.746-7.998). Cox proportional hazard models found a significant association of biomarker-informed AKI subtypes with long-term survival compared with no AKI (adjusted ORs: pooled subclinical and clinical AKI: 1.885, 95% CI 1.003-3.542; combined AKI: 1.792, 95% CI 1.367-2.350).
Conclusions: In the presence or absence of KDIGO clinical criteria for AKI, the urinary NGAL/hepcidin-25-ratio appears to detect prognostically relevant AKI subtypes.
Trial registration number: NCT00672334, clinicaltrials.gov, date of registration: 6th May 2008, https://clinicaltrials.gov/ct2/show/NCT00672334 . Definition of AKI subtypes: subclinical AKI (KDIGO negative AND Ratio-positive), clinical AKI (KDIGO positive AND Ratio-negative) and combined AKI (KDIGO positive AND Ratio-positive) with urinary NGAL/hepcidin-25 ratio-positive cut-off at 85% specificity for in-hospital death. AKI, acute kidney injury. AUC, area under the curve. NGAL, neutrophil gelatinase-associated lipocalin. KDIGO, Kidney Disease Improving Global Outcomes Initiative AKI definition.
Keywords: Cardiopulmonary bypass; Cardiorenal syndrome; NGAL/hepcidin-25 ratio; Subclinical AKI.
© 2021. The Author(s).
Conflict of interest statement
Saban Elitok: None. Prasad Devarajan: This author is a co-inventor on patents submitted for the use of NGAL as a biomarker of kidney injury. Rinaldo Bellomo: None. Berend Isermann: None. Anja Haase-Fielitz: None. Michael Haase: This author is a consultant to FastBiomedical and has received lecture honoraria and travel reimbursement from Siemens Healthcare Diagnostics, Abbott Diagnostics, Roche, Alere, Astute and Baxter on unrelated work.
Figures

Similar articles
-
Urinary Neutrophil Gelatinase-Associated Lipocalin/Hepcidin-25 Ratio for Early Identification of Patients at Risk for Renal Replacement Therapy After Cardiac Surgery: A Substudy of the BICARBONATE Trial.Anesth Analg. 2021 Dec 1;133(6):1510-1519. doi: 10.1213/ANE.0000000000005741. Anesth Analg. 2021. PMID: 34543256 Clinical Trial.
-
Urinary biomarkers may provide prognostic information for subclinical acute kidney injury after cardiac surgery.J Thorac Cardiovasc Surg. 2018 Jun;155(6):2441-2452.e13. doi: 10.1016/j.jtcvs.2017.12.056. Epub 2017 Dec 22. J Thorac Cardiovasc Surg. 2018. PMID: 29366580
-
Predictive Value of Plasma NGAL:Hepcidin-25 for Major Adverse Kidney Events After Cardiac Surgery with Cardiopulmonary Bypass: A Pilot Study.Ann Lab Med. 2021 Jul 1;41(4):357-365. doi: 10.3343/alm.2021.41.4.357. Ann Lab Med. 2021. PMID: 33536353 Free PMC article.
-
Diagnostic value of neutrophil gelatinase-associated lipocalin for early diagnosis of cardiac surgery-associated acute kidney injury: a meta-analysis.Eur J Cardiothorac Surg. 2016 Mar;49(3):746-55. doi: 10.1093/ejcts/ezv199. Epub 2015 Jun 20. Eur J Cardiothorac Surg. 2016. PMID: 26094017 Review.
-
Neutrophil gelatinase-associated lipocalin as a biomarker of acute kidney injury: a critical evaluation of current status.Ann Clin Biochem. 2014 May;51(Pt 3):335-51. doi: 10.1177/0004563214521795. Epub 2014 Feb 11. Ann Clin Biochem. 2014. PMID: 24518531 Free PMC article. Review.
Cited by
-
Advances in laboratory detection of acute kidney injury.Pract Lab Med. 2022 Jun 2;31:e00283. doi: 10.1016/j.plabm.2022.e00283. eCollection 2022 Aug. Pract Lab Med. 2022. PMID: 35677313 Free PMC article.
-
The outcome of acute kidney injury substages based on urinary cystatin C in critically ill children.Ann Intensive Care. 2023 Mar 28;13(1):23. doi: 10.1186/s13613-023-01119-8. Ann Intensive Care. 2023. PMID: 36976367 Free PMC article.
-
Temporary bilateral clamping of renal arteries induces ischemia-reperfusion: A new pig model of acute kidney injury using total intravenous anesthesia.Physiol Rep. 2025 Feb;13(3):e70203. doi: 10.14814/phy2.70203. Physiol Rep. 2025. PMID: 39895016 Free PMC article.
References
-
- Kellum JA, Lameire N, Aspelin P, et al. Kidney disease: improving global outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
-
- Thammathiwat T, Tiranathanagul K, Srisawat N, Susantitaphong P, Praditpornsilpa K, Eiam-Ong S. Clinical and subclinical acute kidney injury in multidrug-resistant septic patients treated with colistimethate sodium: Incidence and clinical outcomes. Nephrology (Carlton) 2020;25:32–39. doi: 10.1111/nep.13663. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
