

Factors indicating intention to vaccinate with a COVID-19 vaccine among older U.S. adults
- PMID: 34029345
- PMCID: PMC8143399
- DOI: 10.1371/journal.pone.0251963
Factors indicating intention to vaccinate with a COVID-19 vaccine among older U.S. adults
Abstract
Background: The success of vaccination efforts to curb the COVID-19 pandemic will require broad public uptake of immunization and highlights the importance of understanding factors associated with willingness to receive a vaccine.
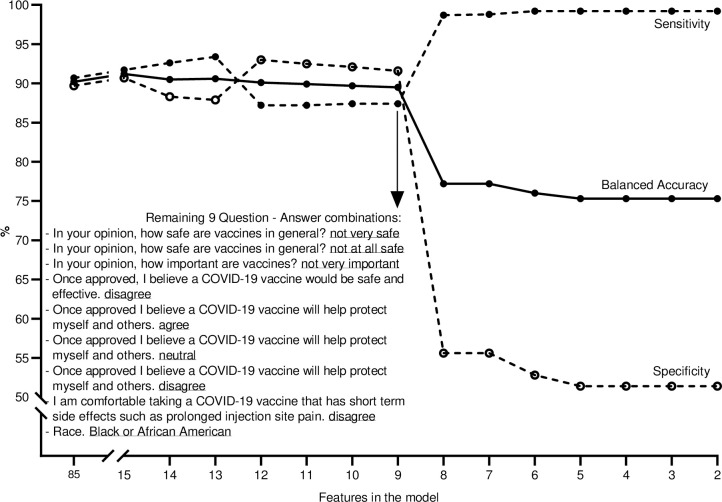
Methods: U.S. adults aged 65 and older enrolled in the HeartlineTM clinical study were invited to complete a COVID-19 vaccine assessment through the HeartlineTM mobile application between November 6-20, 2020. Factors associated with willingness to receive a COVID-19 vaccine were evaluated using an ordered logistic regression as well as a Random Forest classification algorithm.
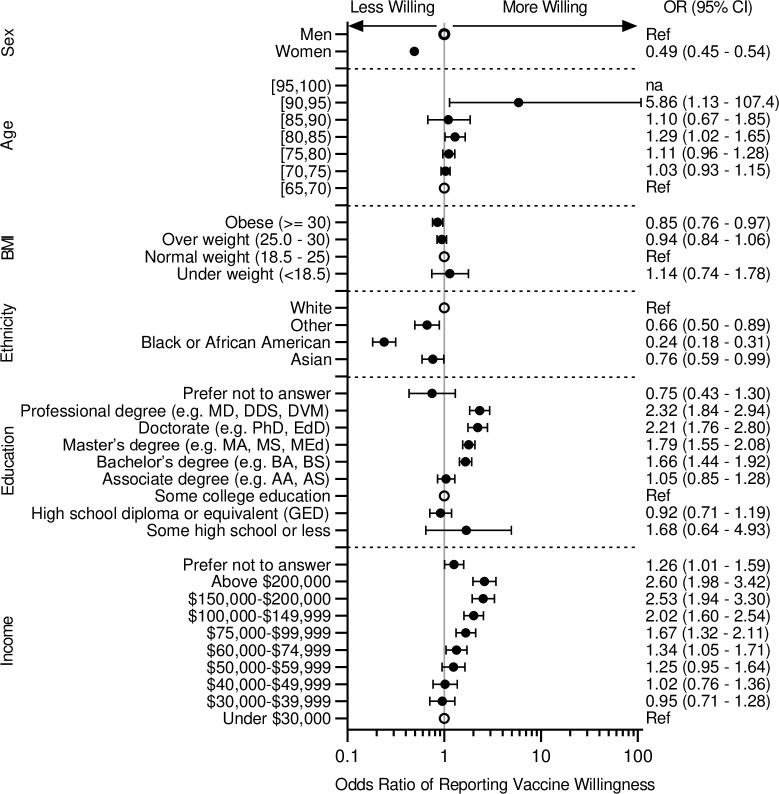
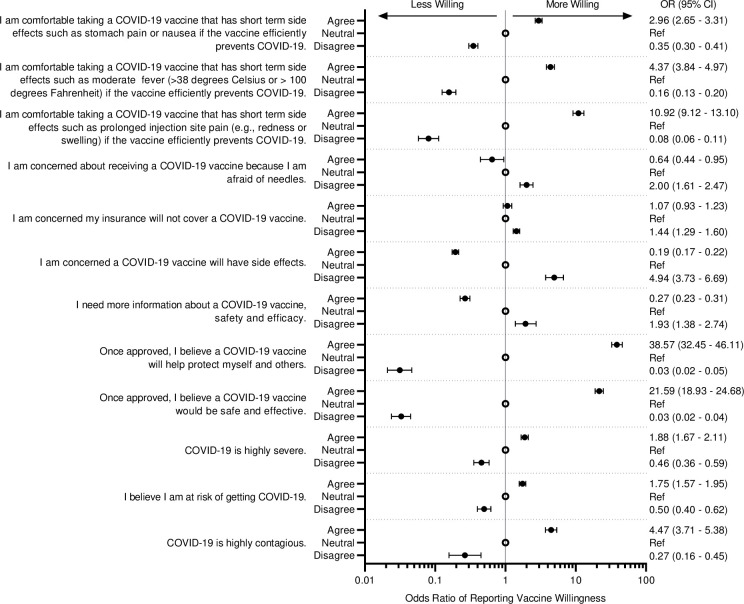
Results: Among 9,106 study participants, 81.3% (n = 7402) responded and had available demographic data. The majority (91.3%) reported a willingness to be vaccinated. Factors most strongly associated with vaccine willingness were beliefs about the safety and efficacy of COVID-19 vaccines and vaccines in general. Women and Black or African American respondents reported lower willingness to vaccinate. Among those less willing to get vaccinated, 66.2% said that they would talk with their health provider before making a decision. During the study, positive results from the first COVID-19 vaccine outcome study were released; vaccine willingness increased after this report.
Conclusions: Even among older adults at high-risk for COVID-19 complications who are participating in a longitudinal clinical study, 1 in 11 reported lack of willingness to receive COVID-19 vaccine in November 2020. Variability in vaccine willingness by gender, race, education, and income suggests the potential for uneven vaccine uptake. Education by health providers directed toward assuaging concerns about vaccine safety and efficacy can help improve vaccine acceptance among those less willing.
Trial registration: Clinicaltrials.gov NCT04276441.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: JN, MK, GJW, JW, TS, JS, PB, RZ, NE, JT, RJ are employees of Janssen and Johnson and Johnson. JN, MK, GJW, JW, TS, JS, PB, RZ, NE, JT, RJ are employees of Janssen and Johnson and Johnson. This does not alter our adherence to PLOS ONE policies on sharing data and materials. JS reports personal fees from Amgen, personal fees from Bayer, personal fees from Merck, personal fees from Novartis, personal fees from Janssen, personal fees from Myokardia, personal fees from Blue Cross Blue Shield of Kansas City, outside the submitted work. In addition, Dr. Spertus has a patent Copyright to the KCCQ with royalties paid and Equity in Health Outcomes Sciences. This does not alter my adherence to PLOS ONE policies on sharing data and materials. MT reports grants from Janssen Inc, personal fees from Medtronic Inc, personal fees from Abbott, grants from Boehringer lngelheim, grants and personal fees from Cardiva Medical, personal fees from iRhythm, grants from Bristol Myers Squibb, grants from American Heart Association, grants from SentreHeart, personal fees from Novartis, personal fees from Biotronik, personal fees from Sanofi, personal fees from Pfizer, grants from Apple, grants from Bayer, personal fees from Myokardia, personal fees from Johnson & Johnson, personal fees from Milestone Pharmaceuticals, outside the submitted work; and Dr. Turakhia is an editor for JAMA Cardiology. This does not alter my adherence to PLOS ONE policies on sharing data and materials. LS reports personal fees from J&J, outside the submitted work. This does not alter my adherence to PLOS ONE policies on sharing data and materials. MG receives research grant support from Janssen. This does not alter my adherence to PLOS ONE policies on sharing data and materials. AMN receives consulting fees from Janssen for serving on the steering committee of the Heartline study. In addition, Dr. Navar receives funding for research to her institution from Amgen and Janssen, and honoraria and consulting fees from Amarin, Amgen, Astra Zeneca, BI, Esperion, Lilly, Sanofi, Regeneron, NovoNordisk, Novartis, The Medicines Company, New Amsterdam, Cerner, 89Bio, and Pfizer, outside the scope of this work. This does not alter my adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Willingness to take COVID-19 vaccination in low-income countries: Evidence from Ethiopia.PLoS One. 2022 Mar 3;17(3):e0264633. doi: 10.1371/journal.pone.0264633. eCollection 2022. PLoS One. 2022. PMID: 35239711 Free PMC article.
-
Factors Associated With Racial/Ethnic Group-Based Medical Mistrust and Perspectives on COVID-19 Vaccine Trial Participation and Vaccine Uptake in the US.JAMA Netw Open. 2021 May 3;4(5):e2111629. doi: 10.1001/jamanetworkopen.2021.11629. JAMA Netw Open. 2021. PMID: 34042990 Free PMC article.
-
Understanding COVID-19 vaccine acceptance in Pakistan: an echo of previous immunizations or prospect of change?Expert Rev Vaccines. 2021 Sep;20(9):1185-1193. doi: 10.1080/14760584.2021.1964963. Epub 2021 Aug 17. Expert Rev Vaccines. 2021. PMID: 34348062
-
Factors Associated with Willingness to be Vaccinated Against COVID-19 in a Large Convenience Sample.J Community Health. 2021 Oct;46(5):1013-1019. doi: 10.1007/s10900-021-00987-0. Epub 2021 Apr 9. J Community Health. 2021. PMID: 33835369 Free PMC article.
-
Willingness to obtain COVID-19 vaccination in adults with multiple sclerosis in the United States.Mult Scler Relat Disord. 2021 Apr;49:102788. doi: 10.1016/j.msard.2021.102788. Epub 2021 Jan 22. Mult Scler Relat Disord. 2021. PMID: 33508570 Free PMC article.
Cited by
-
The Effect of Message Framing on COVID-19 Vaccination Intentions among the Younger Age Population Groups: Results from an Experimental Study in the Italian Context.Vaccines (Basel). 2022 Apr 4;10(4):559. doi: 10.3390/vaccines10040559. Vaccines (Basel). 2022. PMID: 35455307 Free PMC article.
-
Perceptions and Intentions around Uptake of the COVID-19 Vaccination among Older People: A Mixed-Methods Study in Phuket Province, Thailand.Int J Environ Res Public Health. 2023 May 23;20(11):5919. doi: 10.3390/ijerph20115919. Int J Environ Res Public Health. 2023. PMID: 37297522 Free PMC article.
-
Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: A Scoping Review.Vaccines (Basel). 2021 Dec 7;9(12):1445. doi: 10.3390/vaccines9121445. Vaccines (Basel). 2021. PMID: 34960192 Free PMC article.
-
Boosting COVID-19 vaccine inoculation and booster shots: a systematic review and meta-analysis of factors that influence Coronavirus vaccine uptake in practice.Afr Health Sci. 2023 Jun;23(2):3-22. doi: 10.4314/ahs.v23i2.3. Afr Health Sci. 2023. PMID: 38223628 Free PMC article.
-
Assessment of COVID-19 Anxiety Levels and Attitudes to COVID-19 Vaccine among Older Adults in Poland: A Pilot Study.Vaccines (Basel). 2022 Nov 13;10(11):1918. doi: 10.3390/vaccines10111918. Vaccines (Basel). 2022. PMID: 36423014 Free PMC article.
References
-
- Schiavo R. (2020) Vaccine communication in the age of COVID-19: Getting ready for an information war, J Healthc Commun 2020;13:2,73–75. 10.1080/17538068.2020.1778959 - DOI
-
- Cornwall W. Just 50% of Americans plan to get a Covid-19 vaccine. Here’s how to win over the rest. Science. June 30, 2020. (https://www.sciencemag.org/news/2020/06/just-50-americans-plan-get-covid...).
-
- Silverman E. STAT-Harris Poll: The share of Americans interested in getting COVID-19 vaccine as soon as possible is dropping. STAT. October 19, 2020. (https://www.statnews.com/pharmalot/2020/10/19/covid19-coronavirus-pandem...).
-
- Reinhart RJ. More Americans now willing to get COVID-19 vaccine. Gallup. November 17, 2020. (https://news.gallup.com/poll/325208/americans-willing-covid-vaccine.aspx).
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
