

The burden of active infection and anti-SARS-CoV-2 IgG antibodies in the general population: Results from a statewide sentinel-based population survey in Karnataka, India
- PMID: 34029705
- PMCID: PMC8139436
- DOI: 10.1016/j.ijid.2021.05.043
The burden of active infection and anti-SARS-CoV-2 IgG antibodies in the general population: Results from a statewide sentinel-based population survey in Karnataka, India
Abstract
Objective: To estimate the burden of active infection and anti-SARS-CoV-2 IgG antibodies in Karnataka, India, and to assess variation across geographical regions and risk groups.
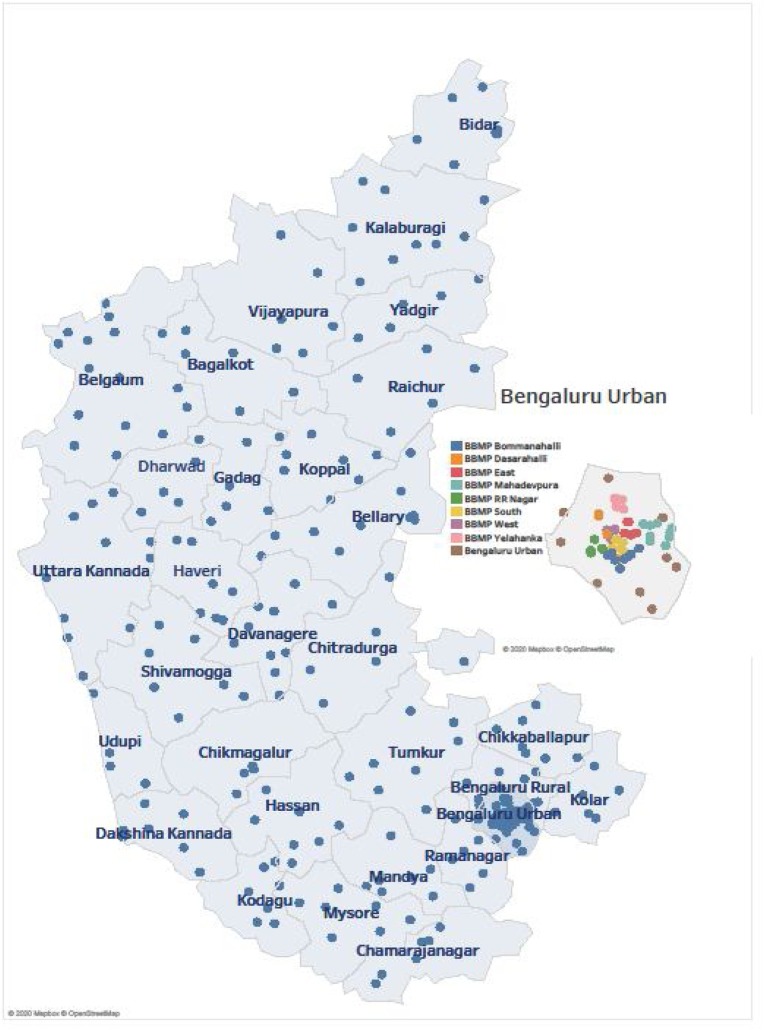
Methods: A cross-sectional survey of 16,416 people covering three risk groups was conducted between 3-16 September 2020 using the state of Karnataka's infrastructure of 290 healthcare facilities across all 30 districts. Participants were further classified into risk subgroups and sampled using stratified sampling. All participants were subjected to simultaneous detection of SARS-CoV-2 IgG using a commercial ELISA kit, SARS-CoV-2 antigen using a rapid antigen detection test (RAT) and reverse transcription-polymerase chain reaction (RT-PCR) for RNA detection. Maximum-likelihood estimation was used for joint estimation of the adjusted IgG, active and total prevalence (either IgG or active or both), while multinomial regression identified predictors.
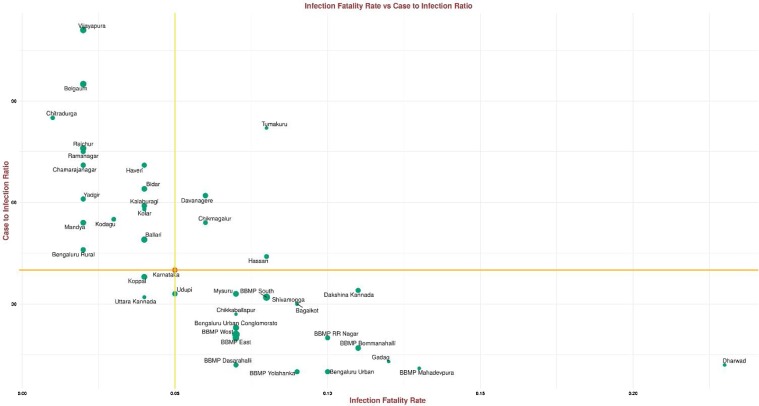
Results: The overall adjusted total prevalence of COVID-19 in Karnataka was 27.7% (95% CI 26.1-29.3), IgG 16.8% (15.5-18.1) and active infection fraction 12.6% (11.5-13.8). The case-to-infection ratio was 1:40 and the infection fatality rate was 0.05%. Influenza-like symptoms or contact with a COVID-19-positive patient were good predictors of active infection. RAT kits had higher sensitivity (68%) in symptomatic people compared with 47% in asymptomatic people.
Conclusion: This sentinel-based population survey was the first comprehensive survey in India to provide accurate estimates of the COVID-19 burden. The findings provide a reasonable approximation of the population immunity threshold levels. Using existing surveillance platforms coupled with a syndromic approach and sampling framework enabled this model to be replicable.
Keywords: Antibody testing; COVID-19; Karnataka; Sentinel survey.
Copyright © 2021. Published by Elsevier Ltd.
Figures
References
-
- Aarti N., Aurnab G., LS S . 2020. Epidemiological and serological surveillance of COVID-19 in Pune city organizations; pp. 1–4. India; Pune.
-
- Chatterjee S., Sarkar A., Karmakar M., Chatterjee S., Paul R. How the asymptomatic population is influencing the COVID-19 outbreak in India? arXiv preprint arXiv. 2020:1–12. 2006.03034.
-
- Financial Express . 2021. Sero-prevalence survey Delhi: here’s why survey result in the capital is’ remarkable’.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
