

Development of a bedside score to predict dengue severity
- PMID: 34030658
- PMCID: PMC8142072
- DOI: 10.1186/s12879-021-06146-z
Development of a bedside score to predict dengue severity
Abstract
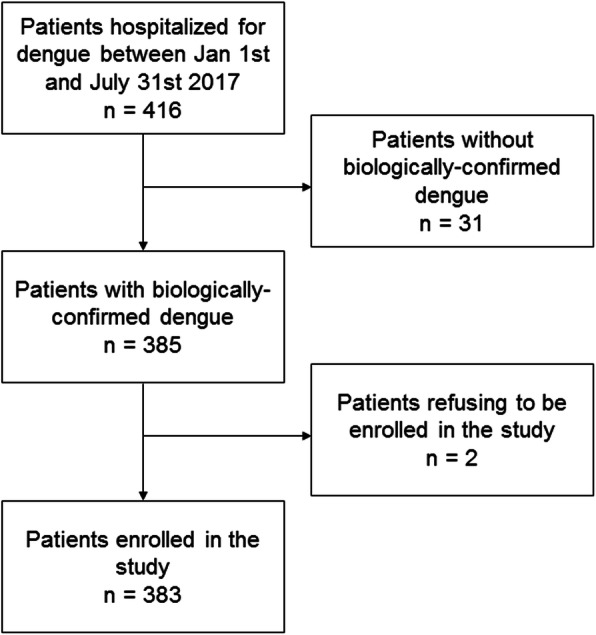
Background: In 2017, New Caledonia experienced an outbreak of severe dengue causing high hospital burden (4379 cases, 416 hospital admissions, 15 deaths). We decided to build a local operational model predictive of dengue severity, which was needed to ease the healthcare circuit.
Methods: We retrospectively analyzed clinical and biological parameters associated with severe dengue in the cohort of patients hospitalized at the Territorial Hospital between January and July 2017 with confirmed dengue, in order to elaborate a comprehensive patient's score. Patients were compared in univariate and multivariate analyses. Predictive models for severity were built using a descending step-wise method.
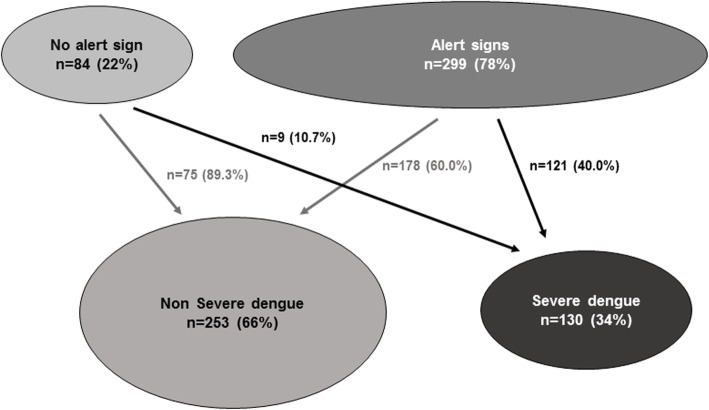
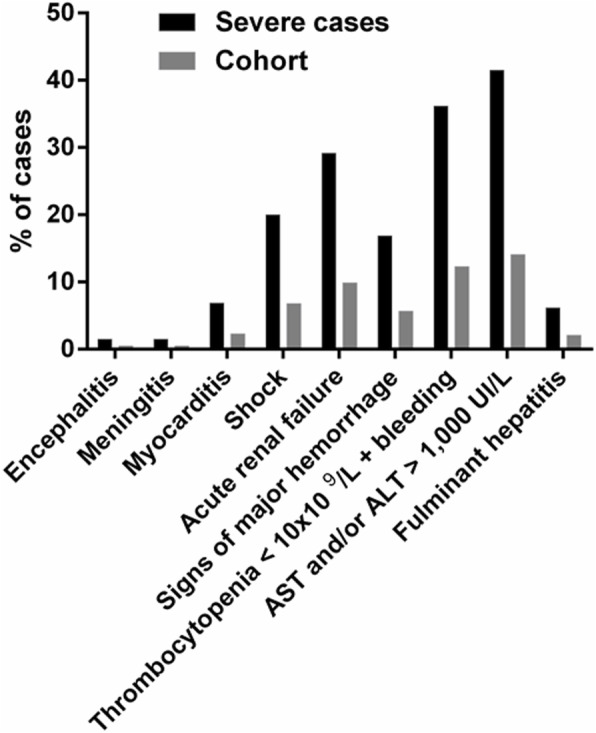
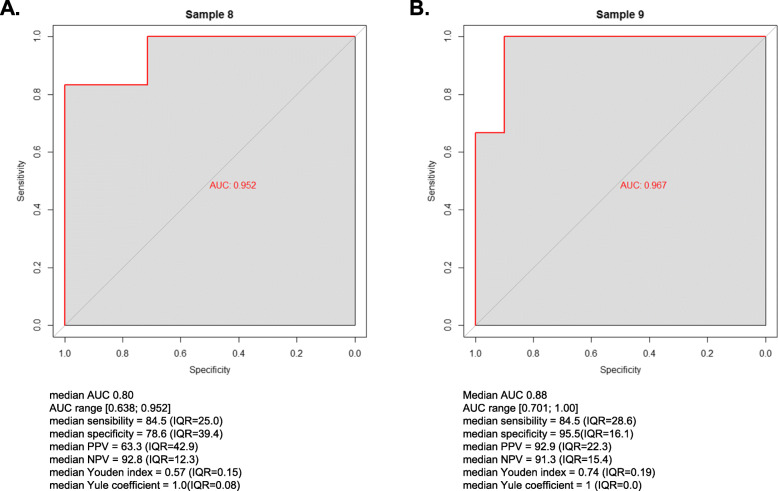
Results: Out of 383 included patients, 130 (34%) developed severe dengue and 13 (3.4%) died. Major risk factors identified in univariate analysis were: age, comorbidities, presence of at least one alert sign, platelets count < 30 × 109/L, prothrombin time < 60%, AST and/or ALT > 10 N, and previous dengue infection. Severity was not influenced by the infecting dengue serotype nor by previous Zika infection. Two models to predict dengue severity were built according to sex. Best models for females and males had respectively a median Area Under the Curve = 0.80 and 0.88, a sensitivity = 84.5 and 84.5%, a specificity = 78.6 and 95.5%, a positive predictive value = 63.3 and 92.9%, a negative predictive value = 92.8 and 91.3%. Models were secondarily validated on 130 patients hospitalized for dengue in 2018.
Conclusion: We built robust and efficient models to calculate a bedside score able to predict dengue severity in our setting. We propose the spreadsheet for dengue severity score calculations to health practitioners facing dengue outbreaks of enhanced severity in order to improve patients' medical management and hospitalization flow.
Keywords: Arboviruses; Dengue; Hospital triage; Operational tool; Pacific; Severity score.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Development and Validation of a Bedside Dengue Severity Score for Predicting Severe Dengue in Children.Indian Pediatr. 2023 May 15;60(5):359-363. doi: 10.1007/s13312-023-2880-7. Epub 2023 Feb 9. Indian Pediatr. 2023. PMID: 36757000 Free PMC article.
-
Factors of severity at admission during an epidemic of dengue 1 in New Caledonia (South Pacific) in 2003.Scand J Infect Dis. 2006;38(8):675-81. doi: 10.1080/00365540600606432. Scand J Infect Dis. 2006. PMID: 16857614
-
Discovery and Validation of Prognostic Biomarker Models to Guide Triage among Adult Dengue Patients at Early Infection.PLoS One. 2016 Jun 10;11(6):e0155993. doi: 10.1371/journal.pone.0155993. eCollection 2016. PLoS One. 2016. PMID: 27286230 Free PMC article.
-
A predictive score for severity in patients with confirmed dengue fever in a tertiary care hospital in Kerala, India.Trans R Soc Trop Med Hyg. 2023 Oct 3;117(10):741-750. doi: 10.1093/trstmh/trad058. Trans R Soc Trop Med Hyg. 2023. PMID: 37625166
-
Diagnostic accuracy and predictive value in differentiating the severity of dengue infection.Trop Med Int Health. 2019 Oct;24(10):1169-1197. doi: 10.1111/tmi.13294. Epub 2019 Aug 19. Trop Med Int Health. 2019. PMID: 31373098 Review.
Cited by
-
Risk Stratification of Dengue Cases Requiring Hospitalization.J Med Virol. 2025 Aug;97(8):e70511. doi: 10.1002/jmv.70511. J Med Virol. 2025. PMID: 40704559 Free PMC article.
-
Prognostic Models in Patients with Dengue: A Systematic Review.Am J Trop Med Hyg. 2025 Feb 11;112(4):898-908. doi: 10.4269/ajtmh.24-0653. Print 2025 Apr 2. Am J Trop Med Hyg. 2025. PMID: 39933179
-
Study of Utility of Basic Arterial Blood Gas Parameters and Lactate as Prognostic Markers in Patients With Severe Dengue.Cureus. 2022 May 3;14(5):e24682. doi: 10.7759/cureus.24682. eCollection 2022 May. Cureus. 2022. PMID: 35663676 Free PMC article.
-
Aspartate Aminotransferase-to-Platelet Ratio Index (APRI) as a Novel Score in Early Detection of Complicated Dengue Fever.J Multidiscip Healthc. 2024 May 16;17:2321-2330. doi: 10.2147/JMDH.S459929. eCollection 2024. J Multidiscip Healthc. 2024. PMID: 38770172 Free PMC article.
-
Viral evolution sustains a dengue outbreak of enhanced severity.Emerg Microbes Infect. 2021 Dec;10(1):536-544. doi: 10.1080/22221751.2021.1899057. Emerg Microbes Infect. 2021. PMID: 33686914 Free PMC article.
References
-
- Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, Drake JM, Brownstein JS, Hoen AG, Sankoh O, Myers MF, George DB, Jaenisch T, Wint GRW, Simmons CP, Scott TW, Farrar JJ, Hay SI. The global distribution and burden of dengue. Nature. 2013;496(7446):504–507. doi: 10.1038/nature12060. - DOI - PMC - PubMed
-
- Sridhar S, Luedtke A, Langevin E, Zhu M, Bonaparte M, Machabert T, Savarino S, Zambrano B, Moureau A, Khromava A, Moodie Z, Westling T, Mascareñas C, Frago C, Cortés M, Chansinghakul D, Noriega F, Bouckenooghe A, Chen J, Ng SP, Gilbert PB, Gurunathan S, DiazGranados CA. Effect of dengue serostatus on dengue vaccine safety and efficacy. N Engl J Med. 2018;379(4):327–340. doi: 10.1056/NEJMoa1800820. - DOI - PubMed
-
- WHO . Dengue: guidelines for diagnosis, treatment, prevention and control: new edition. 2009. - PubMed
-
- WHO Dengue vaccine: WHO position paper – September 2018 – Note de synthèse de l’OMS sur le vaccin contre la dengue– septembre 2018. Wkly Epidemiol Rec. 2018;93(36):457–476.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
