

The inhibition of ABCB1/MDR1 or ABCG2/BCRP enables doxorubicin to eliminate liver cancer stem cells
- PMID: 34031441
- PMCID: PMC8144399
- DOI: 10.1038/s41598-021-89931-9
The inhibition of ABCB1/MDR1 or ABCG2/BCRP enables doxorubicin to eliminate liver cancer stem cells
Abstract
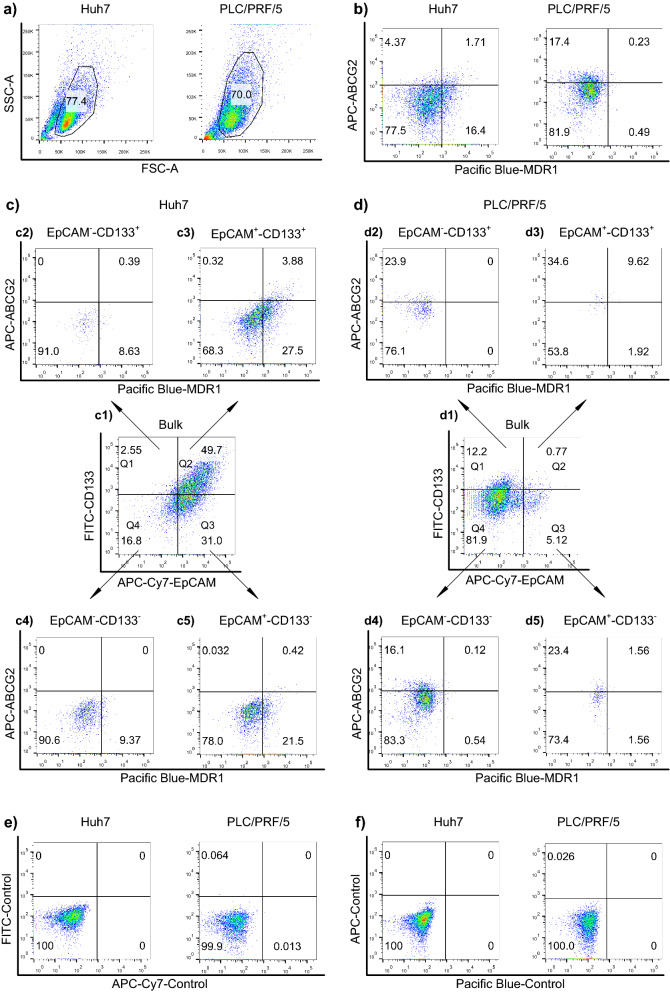
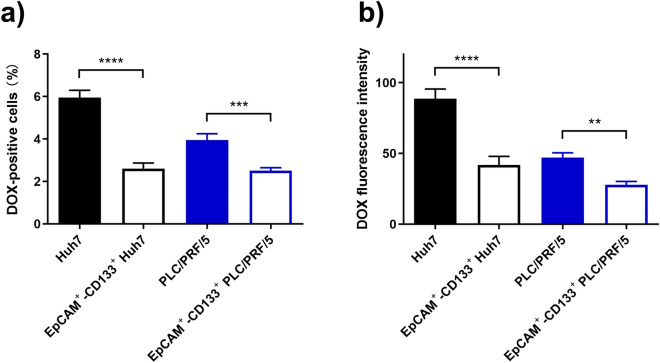
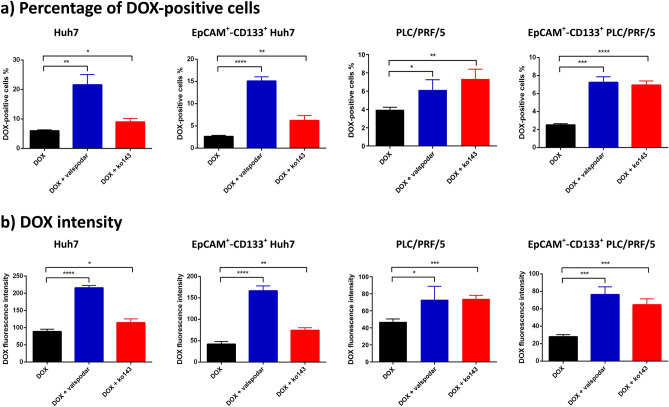
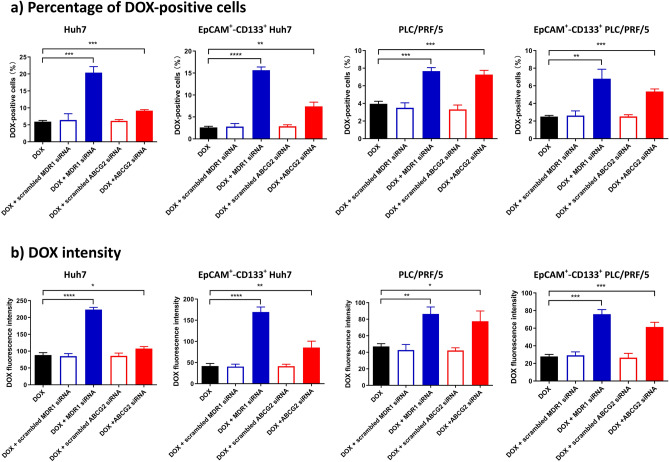
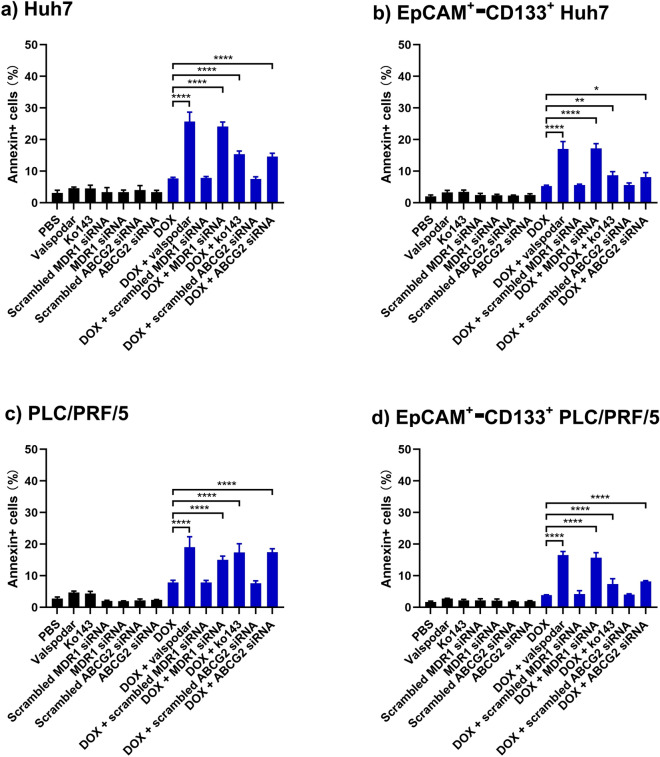
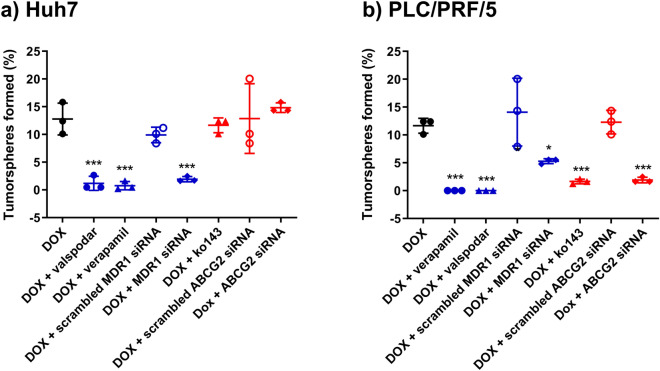
Two ATP-binding cassette transporters, ABCB1/MDR1 and ABCG2/BCRP, are considered the most critical determinants for chemoresistance in hepatocellular carcinoma. However, their roles in the chemoresistance in liver cancer stem cells remain elusive. Here we explored the role of inhibition of MDR1 or ABCG2 in sensitizing liver cancer stem cells to doxorubicin, the most frequently used chemotherapeutic agent in treating liver cancer. We show that the inhibition of MDR1 or ABCG2 in Huh7 and PLC/PRF/5 cells using either pharmacological inhibitors or RNAi resulted in the elevated level of intracellular concentration of doxorubicin and the accompanied increased apoptosis as determined by confocal microscopy, high-performance liquid chromatography, flow cytometry, and annexin V assay. Notably, the inhibition of MDR1 or ABCG2 led to the reversal of the chemoresistance, as evident from the enhanced death of the chemoresistant liver cancer stem cells in tumorsphere-forming assays. Thus, the elevation of effective intracellular concentration of doxorubicin via the inhibition of MDR1 or ABCG2 represents a promising future strategy that transforms doxorubicin from a traditional chemotherapy agent into a robust killer of liver cancer stem cells for patients undergoing transarterial chemoembolization.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Voruciclib, a Potent CDK4/6 Inhibitor, Antagonizes ABCB1 and ABCG2-Mediated Multi-Drug Resistance in Cancer Cells.Cell Physiol Biochem. 2018;45(4):1515-1528. doi: 10.1159/000487578. Epub 2018 Feb 19. Cell Physiol Biochem. 2018. PMID: 29486476
-
An isocorydine derivative (d-ICD) inhibits drug resistance by downregulating IGF2BP3 expression in hepatocellular carcinoma.Oncotarget. 2015 Sep 22;6(28):25149-60. doi: 10.18632/oncotarget.4438. Oncotarget. 2015. PMID: 26327240 Free PMC article.
-
A Novel Synthetic Dihydroindeno[1,2-b] Indole Derivative (LS-2-3j) Reverses ABCB1- and ABCG2-Mediated Multidrug Resistance in Cancer Cells.Molecules. 2018 Dec 10;23(12):3264. doi: 10.3390/molecules23123264. Molecules. 2018. PMID: 30544754 Free PMC article.
-
ABCG2: the key to chemoresistance in cancer stem cells?Expert Opin Drug Metab Toxicol. 2009 Dec;5(12):1529-42. doi: 10.1517/17425250903228834. Expert Opin Drug Metab Toxicol. 2009. PMID: 19708828 Review.
-
Targeting breast cancer resistance protein (BCRP/ABCG2): Functional inhibitors and expression modulators.Eur J Med Chem. 2022 Jul 5;237:114346. doi: 10.1016/j.ejmech.2022.114346. Epub 2022 Apr 6. Eur J Med Chem. 2022. PMID: 35483322 Review.
Cited by
-
P-glycoprotein and cancer: what do we currently know?Heliyon. 2022 Oct 22;8(10):e11171. doi: 10.1016/j.heliyon.2022.e11171. eCollection 2022 Oct. Heliyon. 2022. PMID: 36325145 Free PMC article. Review.
-
Identification and Validation of Prognostic Related Hallmark ATP-Binding Cassette Transporters Associated With Immune Cell Infiltration Patterns in Thyroid Carcinoma.Front Oncol. 2022 Jun 28;12:781686. doi: 10.3389/fonc.2022.781686. eCollection 2022. Front Oncol. 2022. PMID: 35837087 Free PMC article.
-
Mechanism of cancer stemness maintenance in human liver cancer.Cell Death Dis. 2022 Apr 21;13(4):394. doi: 10.1038/s41419-022-04848-z. Cell Death Dis. 2022. PMID: 35449193 Free PMC article. Review.
-
Anticancer Effect of Polyphyllin I in Suppressing Stem Cell-Like Properties of Hepatocellular Carcinoma via the AKT/GSK-3β/β-Catenin Signaling Pathway.Oxid Med Cell Longev. 2022 Oct 22;2022:4031008. doi: 10.1155/2022/4031008. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 36317061 Free PMC article.
-
A Brief Review on Chemoresistance; Targeting Cancer Stem Cells as an Alternative Approach.Int J Mol Sci. 2023 Feb 24;24(5):4487. doi: 10.3390/ijms24054487. Int J Mol Sci. 2023. PMID: 36901917 Free PMC article. Review.
References
-
- Clarke MF. Clinical and therapeutic implications of cancer. Stem Cells. 2019;380:2237–2245. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
