

Testicular involvement of acute lymphoblastic leukemia in children and adolescents: Diagnosis, biology, and management
- PMID: 34031876
- PMCID: PMC9677247
- DOI: 10.1002/cncr.33609
Testicular involvement of acute lymphoblastic leukemia in children and adolescents: Diagnosis, biology, and management
Abstract
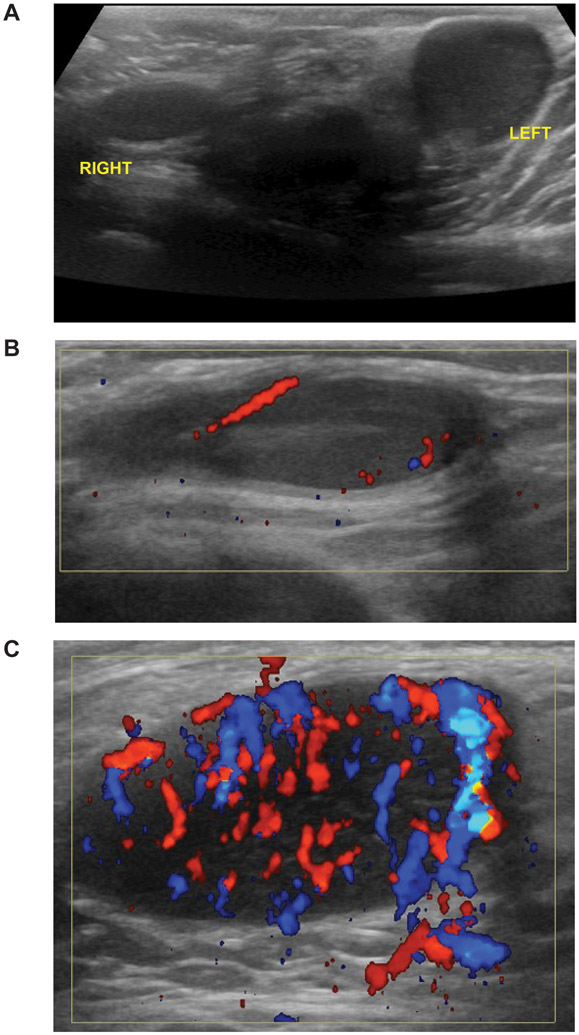
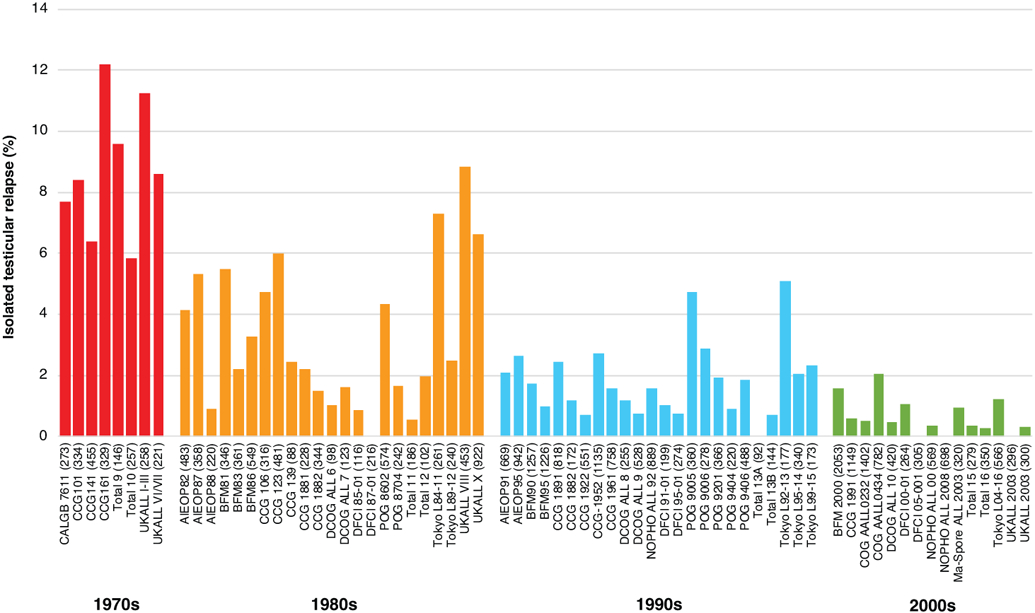
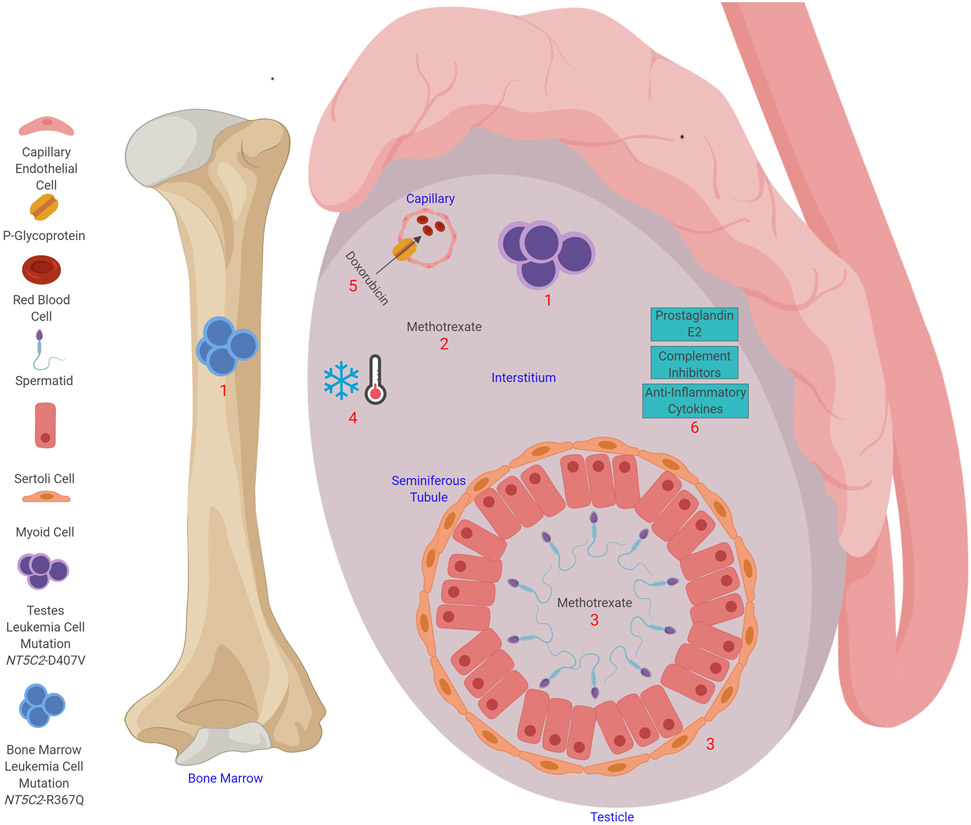
Acute lymphoblastic leukemia (ALL) in children and adolescents can involve the testes at diagnosis or upon relapse. The testes were long considered pharmacologic sanctuary sites, presumably because of the blood-testis barrier, which prevents the entry of large-molecular-weight compounds into the seminiferous tubule. Patients with testicular involvement were historically treated with testicular irradiation or orchiectomy. With the advent of contemporary intensive chemotherapy, including high-dose methotrexate, vincristine/glucocorticoid pulses, and cyclophosphamide, testicular leukemia present at diagnosis can be eradicated, with the risk of testicular relapse being 2% or lower. However, the management of testicular leukemia is not well described in the recent literature and remains relevant in low- and middle-income countries where testicular relapse is still experienced. Chemotherapy can effectively treat late, isolated testicular B-cell ALL relapses without the need for irradiation or orchiectomy in patients with an early response and thereby preserve testicular function. For refractory or early-relapse testicular leukemia, newer treatment approaches such as chimeric antigen receptor-modified T (CAR-T) cell therapy are under investigation. The control of testicular relapse with CAR-T cells and their penetration of the blood-testis barrier have been reported. The outcome of pediatric ALL has been improved remarkably by controlling the disease in the bone marrow, central nervous system, and testes, and such success should be extended globally. LAY SUMMARY: Acute lymphoblastic leukemia (ALL) in children and adolescents can involve the testes at diagnosis or upon relapse. Modern intensive chemotherapy has largely eradicated testicular relapse in high-income countries. Consequently, most current clinicians are not familiar with how to manage it if it does occur, and testicular relapse continues to be a significant problem in low- and middle-income countries that have not had access to modern intensive chemotherapy. The authors review the historical progress made in eradicating testicular ALL and use the lessons learned to make recommendations for treatment.
Keywords: acute lymphoblastic leukemia; adolescents; biology; children; diagnosis; management; testicular leukemia.
© 2021 American Cancer Society.
Conflict of interest statement
Conflicts of interest
All authors have no conflicting interests to declare.
Figures
References
-
- Pui CH, Nichols KE, Yang JJ. Somatic and germline genomics in paediatric acute lymphoblastic leukaemia. Nat Rev Clin Oncol. 2019;16:227–240. - PubMed
-
- Riccardi R, Vigersky RA, Barnes S, Bleyer WA, Poplack DG. Methotrexate levels in the interstitial space and seminiferous tubule of rat testis. Cancer Res. 1982;42:1617–1619. - PubMed
-
- Childhood ALL Collaborative Group. Duration and intensity of maintenance chemotherapy in acute lymphoblastic leukaemia: overview of 42 trials involving 12 000 randomised children. Lancet. 1996;347:1783–1788. - PubMed
-
- Gajjar A, Ribeiro RC, Mahmoud HH, et al. Overt testicular disease at diagnosis is associated with high risk features and a poor prognosis in patients with childhood acute lymphoblastic leukemia. Cancer. 1996;78:2437–2442. - PubMed
-
- Freeman AI, Boyett JM, Glicksman AS, et al. Intermediate-dose methotrexate versus cranial irradiation in childhood acute lymphoblastic leukemia: a ten-year follow-up. Med Pediatr Oncol. 1997;28:98–107. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
