

Procedural Sedation for Pediatric Upper Gastrointestinal Endoscopy in Korea
- PMID: 34032029
- PMCID: PMC8144592
- DOI: 10.3346/jkms.2021.36.e136
Procedural Sedation for Pediatric Upper Gastrointestinal Endoscopy in Korea
Abstract
Background: Sedative upper endoscopy is similar in pediatrics and adults, but it is characteristically more likely to lead to respiratory failure. Although recommended guidelines for pediatric procedural sedation are available within South Korea and internationally, Korean pediatric endoscopists use different drugs, either alone or in combination, in practice. Efforts are being made to minimize the risk of sedation while avoiding procedural challenges. The purpose of this study was to collect and analyze data on the sedation methods used by Korean pediatric endoscopists to help physicians perform pediatric sedative upper endoscopy (PSUE).
Methods: The PSUE procedures performed in 15 Korean pediatric gastrointestinal endoscopic units within a year were analyzed. Drugs used for sedation were grouped according to the method of use, and the depth of sedation was evaluated based on the Ramsay scores. The procedures and their complications were also assessed.
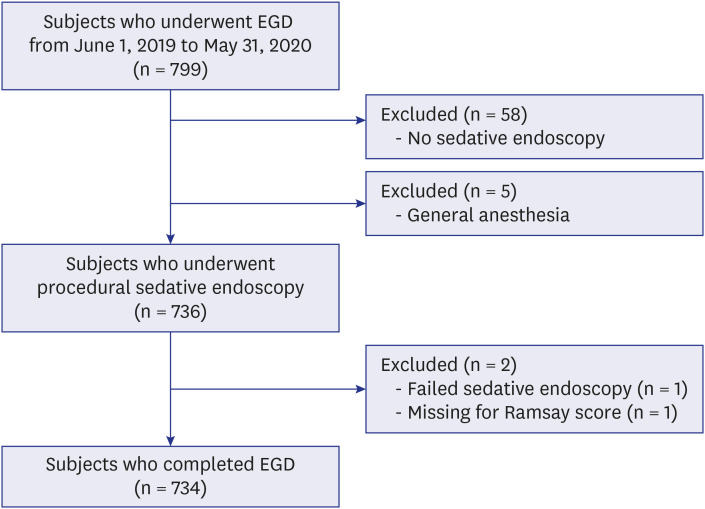
Results: In total, 734 patients who underwent PSUE were included. Sedation and monitoring were performed by an anesthesiologist at one of the institutions. The sedative procedures were performed by a pediatric endoscopist at the other 14 institutions. Regarding the number of assistants present during the procedures, 36.6% of procedures had one assistant, 38.8% had 2 assistants, and 24.5% had 3 assistants. The average age of the patients was 11.6 years old. Of the patients, 19.8% had underlying diseases, 10.0% were taking medications such as epilepsy drugs, and 1.0% had snoring or sleep apnea history. The average duration of the procedures was 5.2 minutes. The subjects were divided into 5 groups as follows: 1) midazolam + propofol + ketamine (M + P + K): n = 18, average dose of 0.03 + 2.4 + 0.5 mg/kg; 2) M + P: n = 206, average dose of 0.06 + 2.1 mg/kg; 3) M + K: n = 267, average dose of 0.09 + 0.69 mg/kg; 4) continuous P infusion for 20 minutes: n = 15, average dose of 6.6 mg/kg; 5) M: n = 228, average dose of 0.11 mg/kg. The average Ramsay score for the five groups was 3.7, with significant differences between the groups (P < 0.001). Regarding the adverse effects, desaturation and increased oxygen supply were most prevalent in the M + K group. Decreases and increases in blood pressure were most prevalent in the M + P + K group, and bag-mask ventilation was most used in the M + K group. There were no reported incidents of intubation or cardiopulmonary resuscitation. A decrease in oxygen saturation was observed in 37 of 734 patients, and it significantly increased in young patients (P = 0.001) and when ketamine was used (P = 0.014). Oxygen saturation was also correlated with dosage (P = 0.037). The use of ketamine (P < 0.001) and propofol (P < 0.001) were identified as factors affecting the Ramsay score in the logistic regression analysis.
Conclusion: Although the drug use by Korean pediatric endoscopists followed the recommended guidelines to an extent, it was apparent that they combined the drugs or reduced the doses depending on the patient characteristics to reduce the likelihood of respiratory failure. Inducing deep sedation facilitates comfort during the procedure, but it also leads to a higher risk of complications.
Keywords: Children; Endoscopy; Ketamine; Midazolam; Propofol; Sedation.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Comment in
-
Letter to the Editor: Optimal Method for Sedation of Pediatric Upper Gastrointestinal Endoscopy.J Korean Med Sci. 2021 Sep 6;36(35):e254. doi: 10.3346/jkms.2021.36.e254. J Korean Med Sci. 2021. PMID: 34490758 Free PMC article. No abstract available.
Similar articles
-
The pediatric sedation unit: a mechanism for pediatric sedation.Pediatrics. 1998 Sep;102(3):E30. doi: 10.1542/peds.102.3.e30. Pediatrics. 1998. PMID: 9724678
-
Comparison of propofol/fentanyl versus ketamine/midazolam for brief orthopedic procedural sedation in a pediatric emergency department.Pediatrics. 2003 Jul;112(1 Pt 1):116-23. doi: 10.1542/peds.112.1.116. Pediatrics. 2003. PMID: 12837876 Clinical Trial.
-
Effects of Sedation Performed by an Anesthesiologist on Pediatric Endoscopy: a Single-Center Retrospective Study in Korea.J Korean Med Sci. 2020 Jun 1;35(21):e183. doi: 10.3346/jkms.2020.35.e183. J Korean Med Sci. 2020. PMID: 32476304 Free PMC article.
-
Endoscopy Sedation Challenges in Patients With Hepatic Encephalopathy: A Focused Review on Propofol and Selective Use of Benzodiazepines.Am J Ther. 2025 May-Jun 01;32(3):e247-e255. doi: 10.1097/MJT.0000000000001926. Epub 2025 Mar 18. Am J Ther. 2025. PMID: 40338682 Review.
-
The Evolution of Sedation for Pediatric Gastrointestinal Endoscopy.Gastrointest Endosc Clin N Am. 2023 Apr;33(2):213-234. doi: 10.1016/j.giec.2022.10.001. Gastrointest Endosc Clin N Am. 2023. PMID: 36948743 Review.
Cited by
-
Effect of Sedation Anesthesia With Intravenous Propofol on Transrectal Ultrasound-Guided Prostate Biopsy Outcomes.J Korean Med Sci. 2022 Apr 18;37(15):e115. doi: 10.3346/jkms.2022.37.e115. J Korean Med Sci. 2022. PMID: 35437964 Free PMC article.
-
Painless Gastrointestinal Endoscopy Assisted with Computed Tomography Image Information Data Monitoring in Postoperative Neurocognitive Dysfunction in Patients with Combined Anesthesia of Propofol and Butorphanol Tartrate under Electronic Health.Comput Math Methods Med. 2022 Jun 20;2022:7086472. doi: 10.1155/2022/7086472. eCollection 2022. Comput Math Methods Med. 2022. PMID: 35770118 Free PMC article.
-
Delayed Adverse Events after Procedural Sedation in Pediatric Patients with Hematologic Malignancies.Medicina (Kaunas). 2022 Sep 2;58(9):1208. doi: 10.3390/medicina58091208. Medicina (Kaunas). 2022. PMID: 36143885 Free PMC article.
-
Practice Patterns of Colorectal Polypectomy in Pediatric Endoscopic Specialists in South Korea: A Nationwide Survey Study.Pediatr Gastroenterol Hepatol Nutr. 2023 Jan;26(1):15-22. doi: 10.5223/pghn.2023.26.1.15. Epub 2023 Jan 10. Pediatr Gastroenterol Hepatol Nutr. 2023. PMID: 36816437 Free PMC article.
-
New sedatives and analgesic drugs for gastrointestinal endoscopic procedures.Clin Endosc. 2022 Sep;55(5):581-587. doi: 10.5946/ce.2021.283. Epub 2022 Aug 29. Clin Endosc. 2022. PMID: 36031764 Free PMC article. Review.
References
-
- Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet. 2006;367(9512):766–780. - PubMed
-
- van Beek EJ, Leroy PL. Safe and effective procedural sedation for gastrointestinal endoscopy in children. J Pediatr Gastroenterol Nutr. 2012;54(2):171–185. - PubMed
-
- Lightdale JR, Mahoney LB, Schwarz SM, Liacouras CA. Methods of sedation in pediatric endoscopy: a survey of NASPGHAN members. J Pediatr Gastroenterol Nutr. 2007;45(4):500–502. - PubMed
-
- Tringali A, Thomson M, Dumonceau JM, Tavares M, Tabbers MM, Furlano R, et al. Pediatric gastrointestinal endoscopy: European Society of Gastrointestinal Endoscopy (ESGE) and European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) guideline executive summary. Endoscopy. 2017;49(1):83–91. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
