

CAVA (Ultrasound-Accelerated Catheter-Directed Thrombolysis on Preventing Post-Thrombotic Syndrome) Trial: Long-Term Follow-Up Results
- PMID: 34032127
- PMCID: PMC8483549
- DOI: 10.1161/JAHA.120.018973
CAVA (Ultrasound-Accelerated Catheter-Directed Thrombolysis on Preventing Post-Thrombotic Syndrome) Trial: Long-Term Follow-Up Results
Abstract
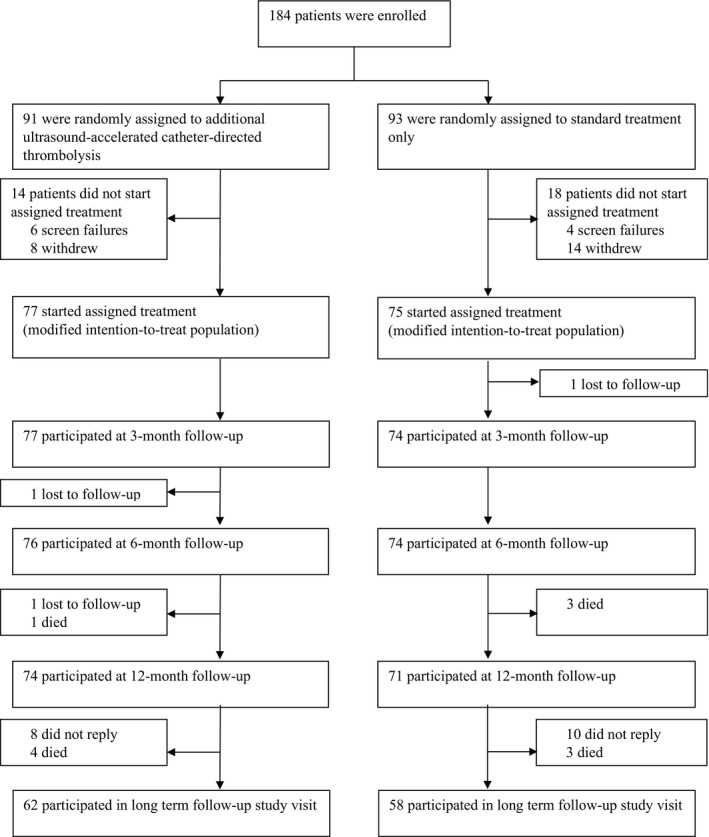
Background The CAVA (Ultrasound-Accelerated Catheter-Directed Thrombolysis Versus Anticoagulation for the Prevention of Post-Thrombotic Syndrome) trial did not show a reduction of post-thrombotic syndrome (PTS) after additional ultrasound-accelerated catheter-directed thrombolysis in patients with acute iliofemoral deep vein thrombosis at 1-year follow-up. This prespecified analysis of the CAVA trial aimed to determine the impact of additional thrombolysis on outcomes of PTS at long-term follow-up. Methods and Results Patients aged 18 to 85 years with a first-time acute iliofemoral deep vein thrombosis were included and randomly assigned (1:1) to either standard treatment plus ultrasound-accelerated catheter-directed thrombolysis or standard treatment alone. The primary outcome was the proportion of PTS (Villalta score ≥5 on 2 occasions ≥3 months apart or venous ulceration) at the final follow-up visit. Additionally, PTS according to the International Society on Thrombosis and Haemostasis (ISTH) consensus definition was assessed to allow external comparability. Major bleedings were the main safety outcome. At a median follow-up of 39.0 months (interquartile range, 23.3-63.8), 120 patients (79.8%) participated in the final follow-up visit: 62 from the intervention group and 58 from the standard treatment group. PTS developed in 19 (30.6%) versus 26 (44.8%) patients, respectively (odds ratio [OR], 0.54; 95% CI, 0.26 to 1.15 [P=0.11]), with an absolute difference between groups of -14.2% (95% CI, -32.0% to 4.8%). Using the ISTH consensus definition, a significant reduction in PTS was observed (29 [46.8%] versus 40 [69.0%]) (OR, 0.40; 95% CI, 0.19-0.84 [P=0.01]) with an absolute difference between groups of -22.2% (95% CI, -39.8% to -2.8%). No new major bleedings occurred following the 12-month follow-up. Conclusions The impact of additional ultrasound-accelerated catheter-directed thrombolysis on the prevention of PTS was found to increase with time. Although this study was limited by its sample size, the overall findings indicate a reduction of mild PTS without impact on quality of life. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT00970619.
Keywords: Iliofemoral deep vein thrombosis; catheter‐directed thrombolysis; long‐term follow‐up; post‐thrombotic syndrome; quality of life.
Conflict of interest statement
Dr Coppens reports grants and personal fees from Bayer Daiichi Sankyo, CSL Behring; grants from Boehringer Ingelheim, Pfizer, Bristol‐Meyers Squibb, and Sanquin Blood Supply; and personal fees from Sobi, NovoNordisk, and UniQure, outside the submitted work. Dr ten Cate reports personal fees and other from Bayer; other from Pfizer and Coagulation profile; and personal fees from LEO Pharma, Gideon Pharmaceuticals, and Alveron Pharma, outside the submitted work. Dr Wittens reports grants from BTG International Group during the conduct of the study. None of the above‐mentioned organizations had any involvement in the design, conduct, analysis, or report of the study data. The remaining authors have no disclosures to report.
Comment in
-
Continuing to Advance the Venous Agenda: Long-Term Insights From the CAVA Trial.J Am Heart Assoc. 2021 Jun;10(11):e021659. doi: 10.1161/JAHA.121.021659. Epub 2021 May 25. J Am Heart Assoc. 2021. PMID: 34032123 Free PMC article. No abstract available.
References
-
- Kahn SR, Shrier I, Julian JA, Ducruet T, Arsenault L, Miron MJ, Roussin A, Desmarais S, Joyal F, Kassis J, et al. Determinants and time course of the postthrombotic syndrome after acute deep venous thrombosis. Ann Intern Med. 2008;149:698–707. DOI: 10.7326/0003-4819-149-10-200811180-00004. - DOI - PubMed
-
- Schulman S, Lindmarker P, Holmstrom M, Larfars G, Carlsson A, Nicol P, Svensson E, Ljungberg B, Viering S, Nordlander S, et al. Post‐thrombotic syndrome, recurrence, and death 10 years after the first episode of venous thromboembolism treated with warfarin for 6 weeks or 6 months. J Thromb Haemost. 2006;4:734–742. DOI: 10.1111/j.1538-7836.2006.01795.x. - DOI - PubMed
-
- Tick LW, Doggen CJ, Rosendaal FR, Faber WR, Bousema MT, Mackaay AJ, van Balen P, Kramer MH. Predictors of the post‐thrombotic syndrome with non‐invasive venous examinations in patients 6 weeks after a first episode of deep vein thrombosis. J Thromb Haemost. 2010;8:2685–2692. DOI: 10.1111/j.1538-7836.2010.04065.x. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
