

Clinical indications of premenstrual disorders and subsequent risk of injury: a population-based cohort study in Sweden
- PMID: 34034729
- PMCID: PMC8152351
- DOI: 10.1186/s12916-021-01989-4
Clinical indications of premenstrual disorders and subsequent risk of injury: a population-based cohort study in Sweden
Abstract
Background: Premenstrual disorders, including premenstrual syndrome and premenstrual dysphoric disorder, are suggested to be correlated with suicidal behavior and accidents in cross-sectional and retrospective studies. However, prospective data are still lacking.
Methods: We performed a population-based cohort study including 1,472,379 Swedish women of reproductive age who were followed from 2001 to 2012. Within the cohort, we also performed a sibling analysis where we compared the rates of injury between full sisters. By linking to the Patient and the Prescribed Drug Registers, we identified 18,628 women with any clinical indications for premenstrual disorders in the cohort (population analysis) and 7674 women in the sibling analysis. Any injury, primarily suicidal behavior (completed suicide and suicide attempt) or accidents (e.g., fall and transportation accidents), was identified through the Patient and Causes of Death Registers as the primary outcome. We estimated hazard ratios (HRs) and 95% confidence intervals (CIs) of these outcomes among women with premenstrual disorders in both population and sibling analyses using multivariable Cox proportional hazards regression.
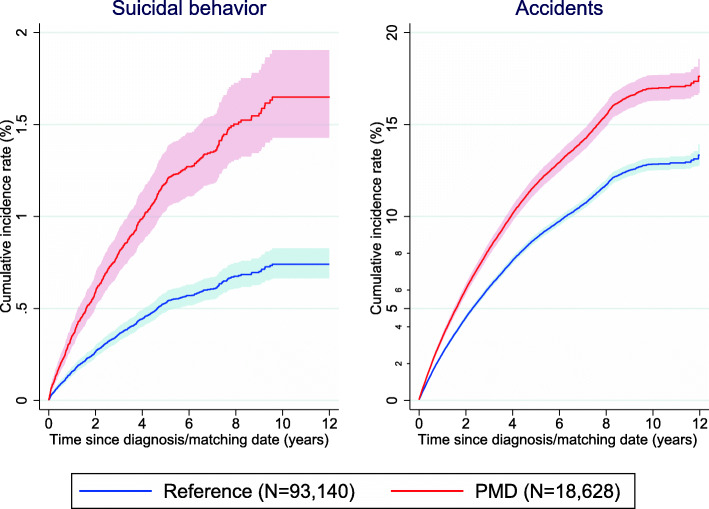
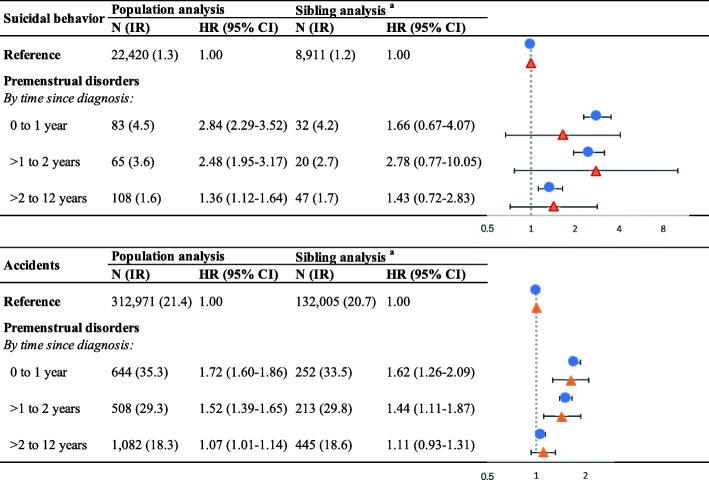
Results: During a maximal follow-up of 12 years (mean 9.55 years), we identified 2390 women with premenstrual disorders with any injury; 216 through suicidal behavior and 2191 through accidents. Compared to women without premenstrual disorders, women with premenstrual disorders were at increased risk of any injury (HR 1.37, 95% CI 1.31-1.42), particularly suicidal behavior (HR 2.26, 95% CI 1.97-2.59) and accidents (HR 1.32, 95% CI 1.27-1.38). Such associations somewhat attenuated yet remained significant in the sibling analysis (HRs: 1.31 for any injury, 1.86 for suicidal behavior, and 1.29 for accidents). Additional adjustment for psychiatric comorbidities minimally altered the associations with any injury and accidents in both population and sibling analyses, whereas the association with suicidal behavior was considerably attenuated to non-significance in the sibling analysis. Such risks were particularly strong within 2 years after receiving the diagnosis of premenstrual disorders and were evident among women with premenstrual disorders with and without psychiatric comorbidities.
Conclusions: Our findings suggest that women with a clinical indication of premenstrual disorders are at increased subsequent risk of injury, particularly accidents within the first 2 years after diagnosis.
Keywords: Accidents; Cohort study; Injury; Premenstrual disorders; Suicidal behavior.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Use of hormonal contraceptives and antidepressants and risks of suicidal behavior and accidents among women with premenstrual disorders: a nationwide cohort study.BMC Med. 2022 Dec 15;20(1):482. doi: 10.1186/s12916-022-02671-z. BMC Med. 2022. PMID: 36522649 Free PMC article.
-
Mortality Risk Among Women With Premenstrual Disorders in Sweden.JAMA Netw Open. 2024 May 1;7(5):e2413394. doi: 10.1001/jamanetworkopen.2024.13394. JAMA Netw Open. 2024. PMID: 38805225 Free PMC article.
-
The bidirectional association between premenstrual disorders and perinatal depression: A nationwide register-based study from Sweden.PLoS Med. 2024 Mar 28;21(3):e1004363. doi: 10.1371/journal.pmed.1004363. eCollection 2024 Mar. PLoS Med. 2024. PMID: 38547436 Free PMC article.
-
Suicide attempt and death by suicide among parents of young individuals with cancer: A population-based study in Denmark and Sweden.PLoS Med. 2024 Jan 16;21(1):e1004322. doi: 10.1371/journal.pmed.1004322. eCollection 2024 Jan. PLoS Med. 2024. PMID: 38227561 Free PMC article.
-
Perinatal Depression and Risk of Suicidal Behavior.JAMA Netw Open. 2024 Jan 2;7(1):e2350897. doi: 10.1001/jamanetworkopen.2023.50897. JAMA Netw Open. 2024. PMID: 38194232 Free PMC article.
Cited by
-
Altered visual cortex excitability in premenstrual dysphoric disorder: Evidence from magnetoencephalographic gamma oscillations and perceptual suppression.PLoS One. 2022 Dec 30;17(12):e0279868. doi: 10.1371/journal.pone.0279868. eCollection 2022. PLoS One. 2022. PMID: 36584199 Free PMC article.
-
Premenstrual disorders and risk of cardiovascular diseases.Nat Cardiovasc Res. 2025 Aug;4(8):1001-1010. doi: 10.1038/s44161-025-00684-4. Epub 2025 Jul 11. Nat Cardiovasc Res. 2025. PMID: 40646267 Free PMC article.
-
Prevalence and correlates of current suicidal ideation in women with premenstrual dysphoric disorder.BMC Womens Health. 2022 Feb 11;22(1):35. doi: 10.1186/s12905-022-01612-5. BMC Womens Health. 2022. PMID: 35148753 Free PMC article. Clinical Trial.
-
Use of hormonal contraceptives and antidepressants and risks of suicidal behavior and accidents among women with premenstrual disorders: a nationwide cohort study.BMC Med. 2022 Dec 15;20(1):482. doi: 10.1186/s12916-022-02671-z. BMC Med. 2022. PMID: 36522649 Free PMC article.
-
Mortality Risk Among Women With Premenstrual Disorders in Sweden.JAMA Netw Open. 2024 May 1;7(5):e2413394. doi: 10.1001/jamanetworkopen.2024.13394. JAMA Netw Open. 2024. PMID: 38805225 Free PMC article.
References
-
- ACOG. Premenstual Syndrome (PMS) May, 2015 [Available from: https://www.acog.org/womens-health/faqs/premenstrual-syndrome.
-
- Association AP. Diagnostic and statistical manual of mental disorders (5th ed.). 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
