

Aortic dissection diagnosed on stroke computed tomography protocol: a case report
- PMID: 34034814
- PMCID: PMC8152142
- DOI: 10.1186/s13256-021-02850-1
Aortic dissection diagnosed on stroke computed tomography protocol: a case report
Abstract
Background: Aortic dissection is one of the causes of stroke. Because cerebral infarction with aortic dissection is a contraindication to intravenous recombinant tissue plasminogen activator (rt-PA) therapy, exclusion of aortic dissection is necessary prior to its administration. However, imaging takes time to provide a diagnosis, possibly causing delays in surgical treatment.
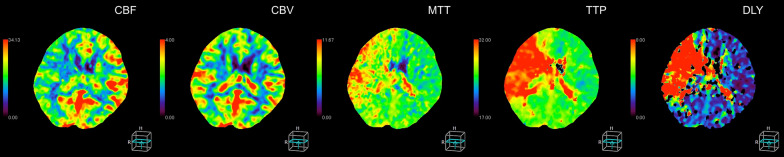
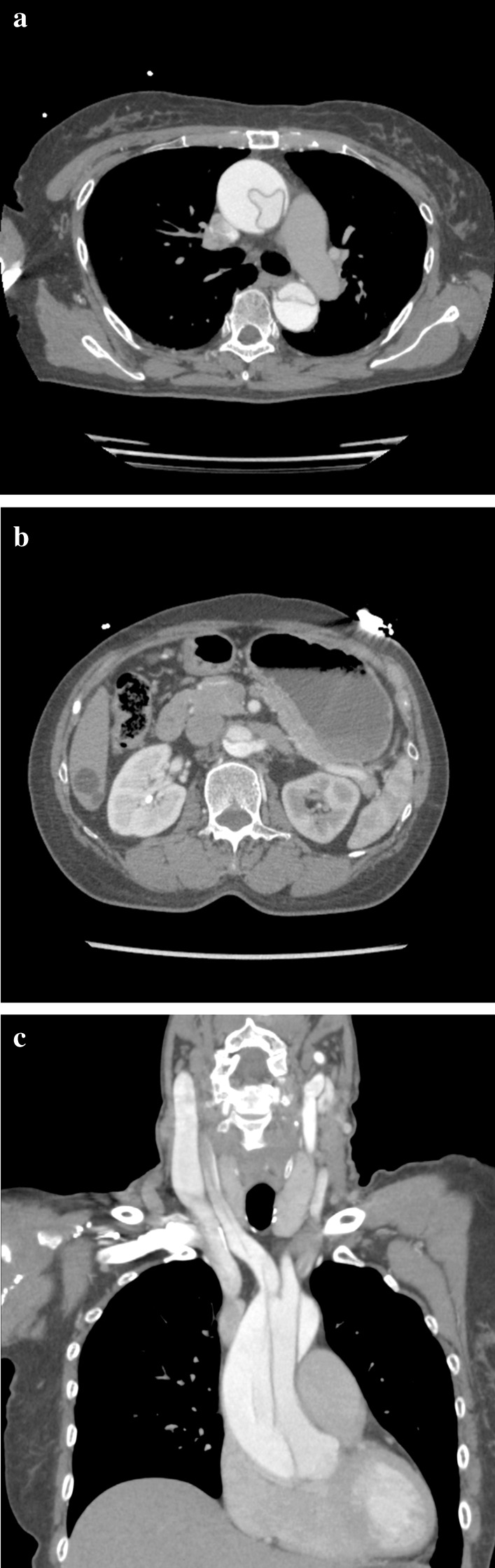
Case presentation: A 65-year-old Japanese female patient was transported to the hospital for a suspected stroke, with back pain and left upper and lower extremity palsy which occurred while eating. Upon arrival at the hospital, the left lower limb paralysis had improved, but the left upper limb paralysis remained. Right back pain had also developed. A plain head computed tomography (CT) scan performed 110 minutes after onset showed no acute bleeding or infarction. Subsequent CT perfusion (CTP) showed acute perfusion disturbance in the right hemisphere without infarction, known as ischemic penumbra. The four-dimensional maximum-intensity projection image reconstructed from CTP showed a delayed enhancement at the right internal carotid and right middle cerebral arteries compared to the contralateral side, suggesting a proximal vascular lesion. Contrast helical CT from the neck to abdomen revealed an acute aortic dissection of Stanford type A with false lumen patency. The dissection extended to the proximal right common carotid artery. The patient underwent an emergency total arch replacement and open stent graft. After recovering well, the patient was ambulatory upon discharge from the hospital. The combination of plain head CT, CTP, and helical CT scan from the neck to abdomen enabled us to evaluate for stroke and aortic dissection within a short amount of time, allowing for early therapeutic intervention.
Conclusions: When acute stroke is suspected due to neurological deficits, plain head CT is the first choice for imaging diagnosis. The addition of cervical CT angiography can reliably exclude stroke due to aortic dissection. CTP can identify ischemic penumbra, which cannot be diagnosed by plain head CT or diffusion-weighted magnetic resonance imaging. These combined stroke CT protocols helped us avoid missing an aortic dissection.
Keywords: Acute aortic dissociation; Acute cerebral infarction; Computed tomography perfusion; Stroke.
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
[A case of brain infarction and thoracic aortic dissection without chest nor back pain diagnosed by carotid duplex ultrasonography].Rinsho Shinkeigaku. 2009 Feb-Mar;49(2-3):104-8. doi: 10.5692/clinicalneurol.49.104. Rinsho Shinkeigaku. 2009. PMID: 19348175 Japanese.
-
Stanford type a aortic dissection with cerebral infarction: a rare case report.BMC Neurol. 2020 Jun 23;20(1):253. doi: 10.1186/s12883-020-01832-y. BMC Neurol. 2020. PMID: 32576285 Free PMC article.
-
[A case of acute aortic dissection presenting with cerebral ischemic symptoms: utility of 3D CT angiography and CT perfusion for the diagnosis of acute stroke].Brain Nerve. 2014 Aug;66(8):1001-5. Brain Nerve. 2014. PMID: 25082322 Japanese.
-
Acute ischemic stroke as a complication of Stanford type A acute aortic dissection: a review and proposed clinical recommendations for urgent diagnosis.Gen Thorac Cardiovasc Surg. 2018 Aug;66(8):439-445. doi: 10.1007/s11748-018-0956-4. Epub 2018 Jun 13. Gen Thorac Cardiovasc Surg. 2018. PMID: 29948797 Review.
-
[Delayed Diagnosis of Aortic Dissection Following Thrombolytic Therapy in a Patient with Acute Ischemic Stroke;Report of a Case].Kyobu Geka. 2016 Nov;69(12):1037-1040. Kyobu Geka. 2016. PMID: 27821831 Review. Japanese.
Cited by
-
Transient Neurological Deficits in a Patient With Prior DeBakey Type 1 Aortic Dissection.Cureus. 2024 Aug 26;16(8):e67839. doi: 10.7759/cureus.67839. eCollection 2024 Aug. Cureus. 2024. PMID: 39328642 Free PMC article.
-
Stenting in Brain Hemodynamic Injury of Carotid Origin Caused by Type A Aortic Dissection: Local Experience and Systematic Literature Review.J Pers Med. 2022 Dec 27;13(1):58. doi: 10.3390/jpm13010058. J Pers Med. 2022. PMID: 36675719 Free PMC article.
-
Neurological Manifestations of Aortic Dissection: A Scoping Review.J Acute Med. 2024 Dec 1;14(4):135-144. doi: 10.6705/j.jacme.202412_14(4).0001. J Acute Med. 2024. PMID: 39624147 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
