

Single-Cell Characterization of the Immune Microenvironment of Melanoma Brain and Leptomeningeal Metastases
- PMID: 34035069
- PMCID: PMC8282775
- DOI: 10.1158/1078-0432.CCR-21-1694
Single-Cell Characterization of the Immune Microenvironment of Melanoma Brain and Leptomeningeal Metastases
Abstract
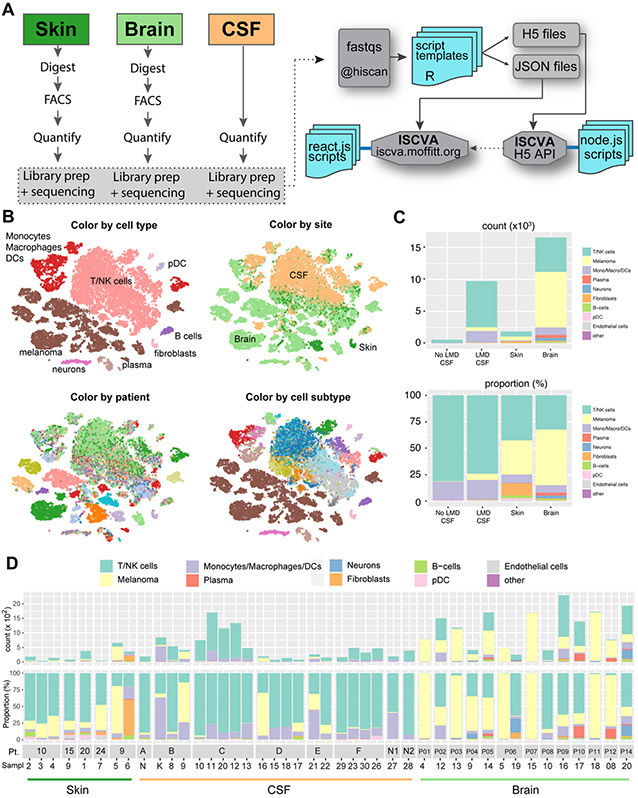
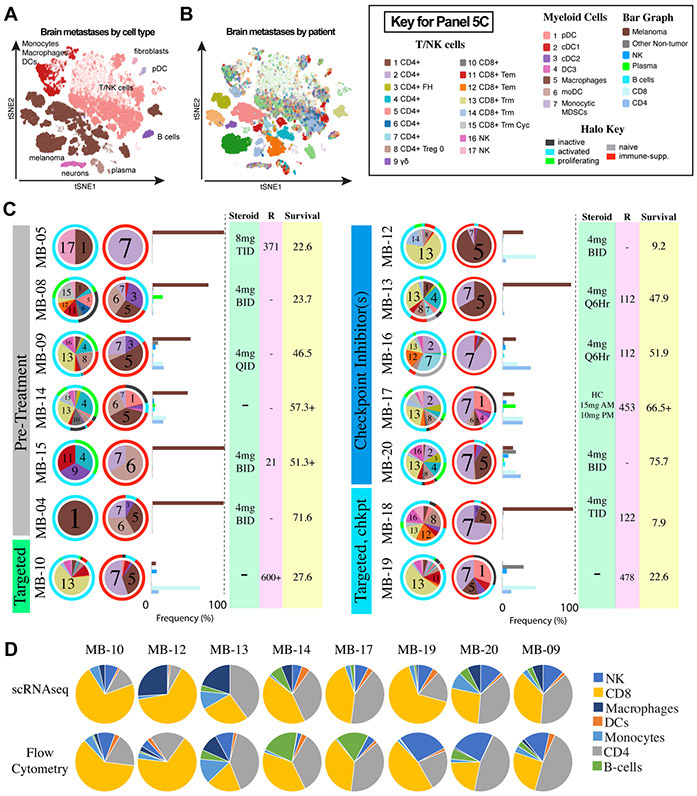
Purpose: Melanoma brain metastases (MBM) and leptomeningeal melanoma metastases (LMM) are two different manifestations of melanoma CNS metastasis. Here, we used single-cell RNA sequencing (scRNA-seq) to define the immune landscape of MBM, LMM, and melanoma skin metastases.
Experimental design: scRNA-seq was undertaken on 43 patient specimens, including 8 skin metastases, 14 MBM, and 19 serial LMM specimens. Detailed cell type curation was performed, the immune landscapes were mapped, and key results were validated by IHC and flow cytometry. Association analyses were undertaken to identify immune cell subsets correlated with overall survival.
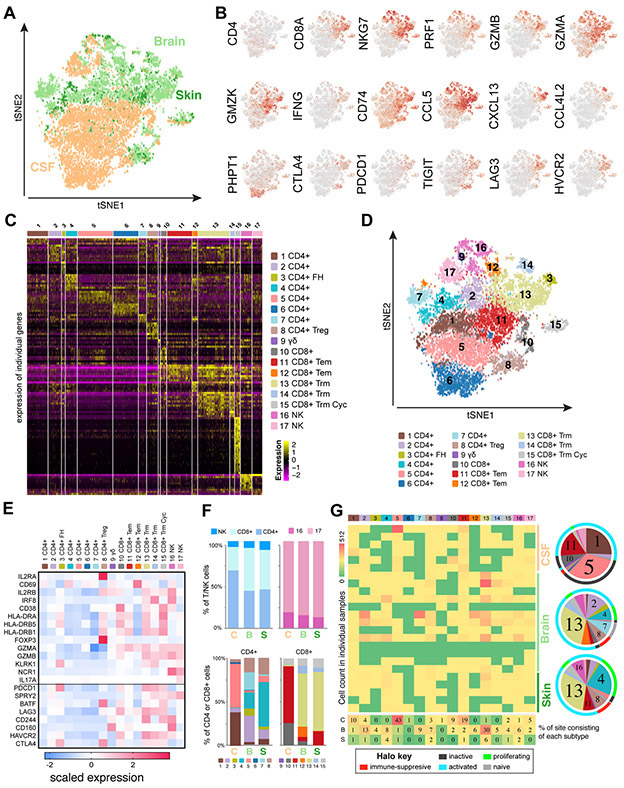
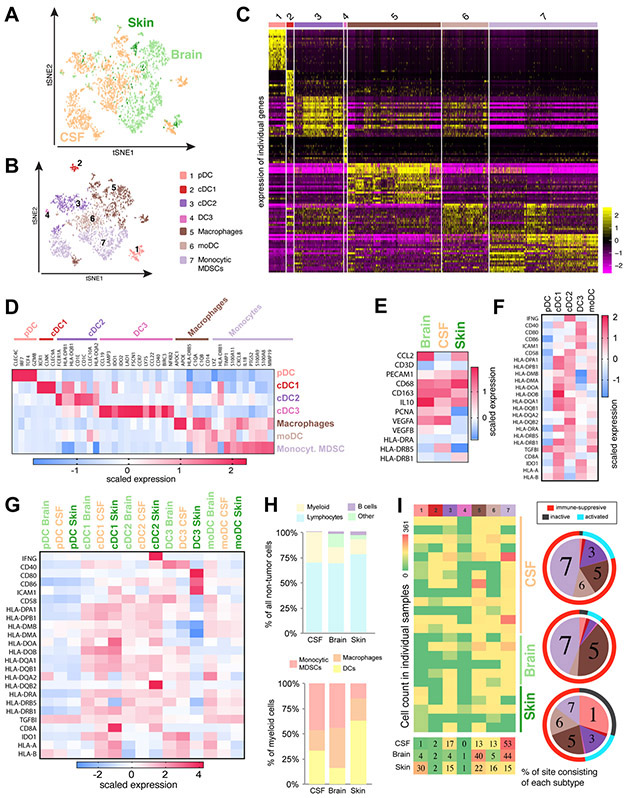
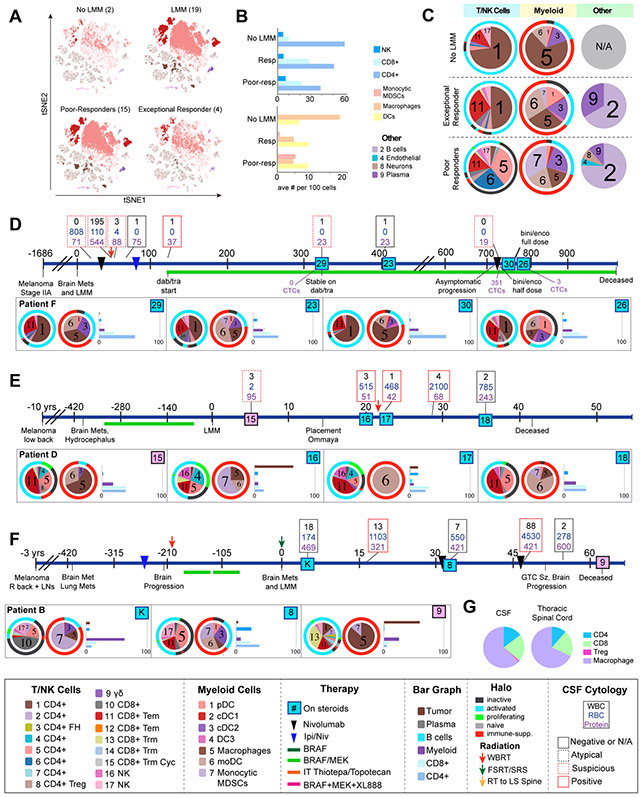
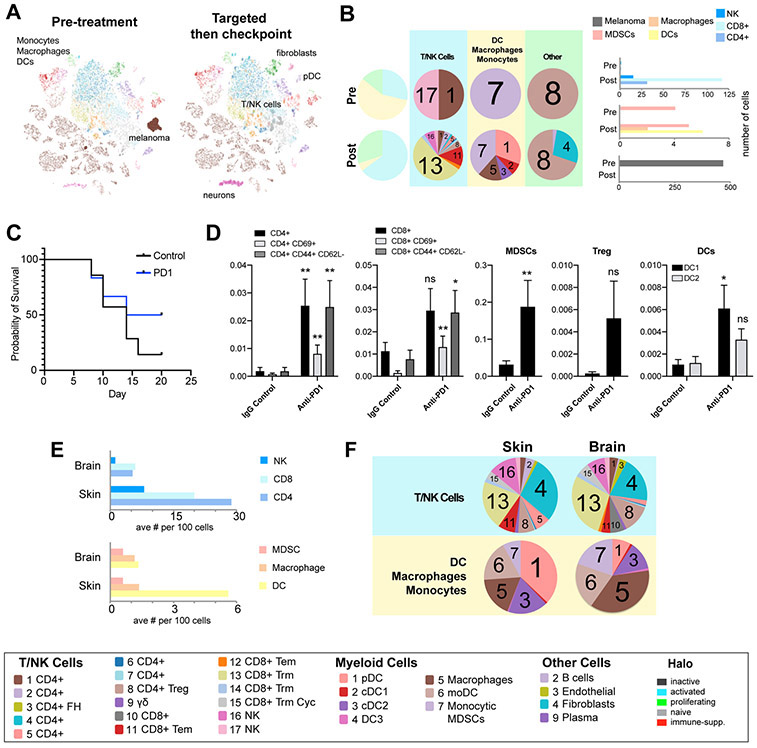
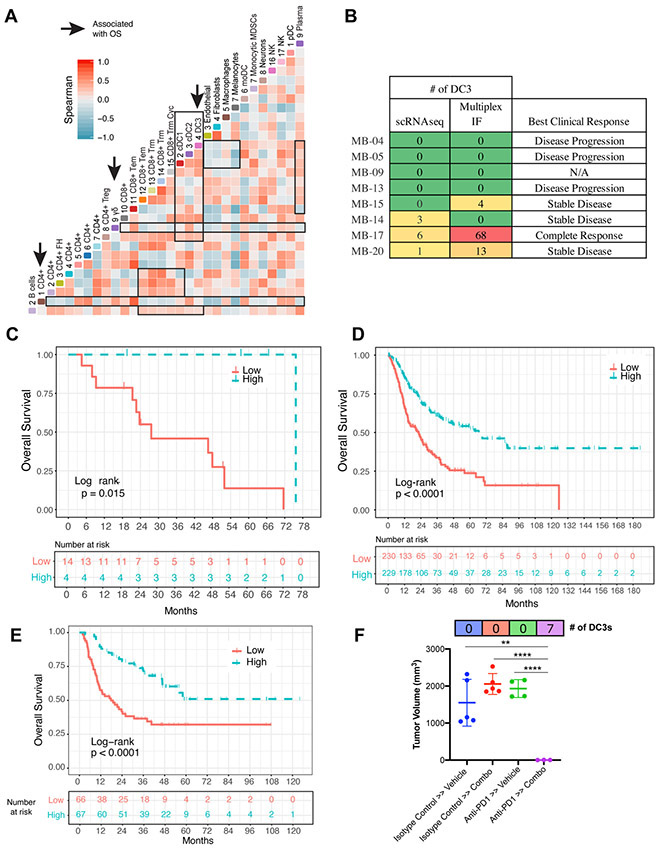
Results: The LMM microenvironment was characterized by an immune-suppressed T-cell landscape distinct from that of brain and skin metastases. An LMM patient with long-term survival demonstrated an immune repertoire distinct from that of poor survivors and more similar to normal cerebrospinal fluid (CSF). Upon response to PD-1 therapy, this extreme responder showed increased levels of T cells and dendritic cells in their CSF, whereas poor survivors showed little improvement in their T-cell responses. In MBM patients, therapy led to increased immune infiltrate, with similar T-cell transcriptional diversity noted between skin metastases and MBM. A correlation analysis across the entire immune landscape identified the presence of a rare population of dendritic cells (DC3) that was associated with increased overall survival and positively regulated the immune environment through modulation of activated T cells and MHC expression.
Conclusions: Our study provides the first atlas of two distinct sites of melanoma CNS metastases and defines the immune cell landscape that underlies the biology of this devastating disease.
©2021 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Balch CM. Cutaneous melanoma. St. Louis, Mo.: Quality Medical Pub.; 2003. xxiii, 799 p. p.
-
- Kenchappa RS, Tran N, Rao NG, Smalley KS, Gibney GT, Sondak VK, et al. Novel Treatments for Melanoma Brain Metastases. Cancer Control 2013;20(4):298–306. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
