

Association of socioeconomic status with medical assistance in dying: a case-control analysis
- PMID: 34035092
- PMCID: PMC8154947
- DOI: 10.1136/bmjopen-2020-043547
Association of socioeconomic status with medical assistance in dying: a case-control analysis
Abstract
Objectives: Economic constraints are a common explanation of why patients with low socioeconomic status tend to experience less access to medical care. We tested whether the decreased care extends to medical assistance in dying in a healthcare system with no direct economic constraints.
Design: Population-based case-control study of adults who died.
Setting: Ontario, Canada, between 1 June 2016 and 1 June 2019.
Patients: Patients receiving palliative care under universal insurance with no user fees.
Exposure: Patient's socioeconomic status identified using standardised quintiles.
Main outcome measure: Whether the patient received medical assistance in dying.
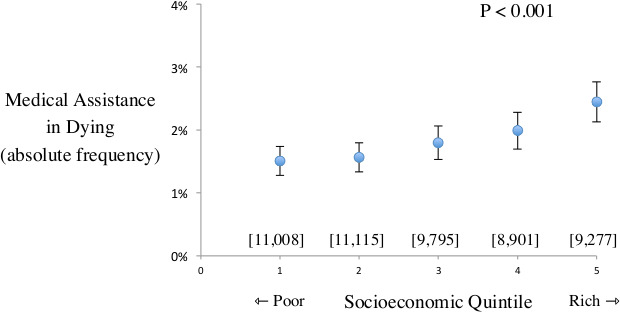
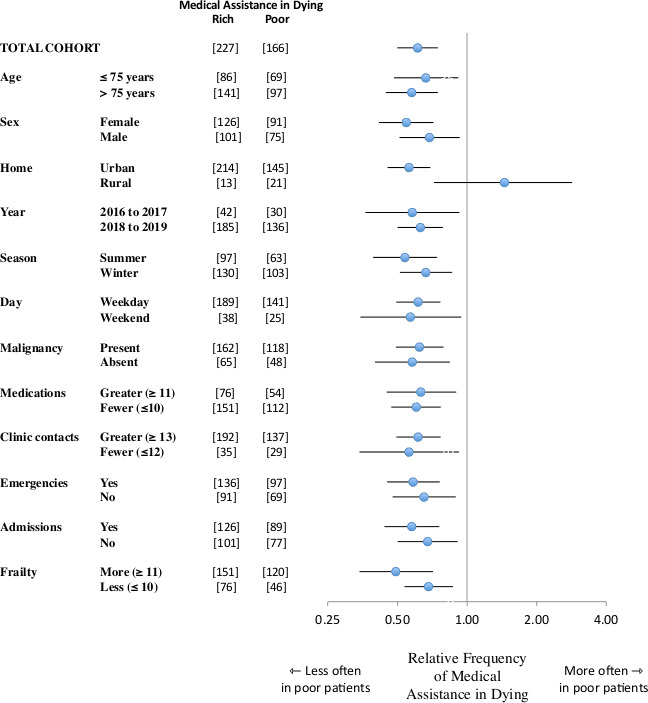
Results: A total of 50 096 palliative care patients died, of whom 920 received medical assistance in dying (cases) and 49 176 did not receive medical assistance in dying (controls). Medical assistance in dying was less frequent for patients with low socioeconomic status (166 of 11 008=1.5%) than for patients with high socioeconomic status (227 of 9277=2.4%). This equalled a 39% decreased odds of receiving medical assistance in dying associated with low socioeconomic status (OR=0.61, 95% CI 0.50 to 0.75, p<0.001). The relative decrease was evident across diverse patient groups and after adjusting for age, sex, home location, malignancy diagnosis, healthcare utilisation and overall frailty. The findings also replicated in a subgroup analysis that matched patients on responsible physician, a sensitivity analysis based on a different socioeconomic measure of low-income status and a confirmation study using a randomised survey design.
Conclusions: Patients with low socioeconomic status are less likely to receive medical assistance in dying under universal health insurance. An awareness of this imbalance may help in understanding patient decisions in less extreme clinical settings.
Keywords: adult palliative care; cancer pain; health policy; primary care; rationing.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Nicol J, Tiedemann M. Bill C-14: an act to amend the criminal code and to make related amendments to other acts (medical assistance in dying. Ottawa: Library of Parliament, 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical