

Impact of mobile stroke units
- PMID: 34035130
- PMCID: PMC8292607
- DOI: 10.1136/jnnp-2020-324005
Impact of mobile stroke units
Abstract
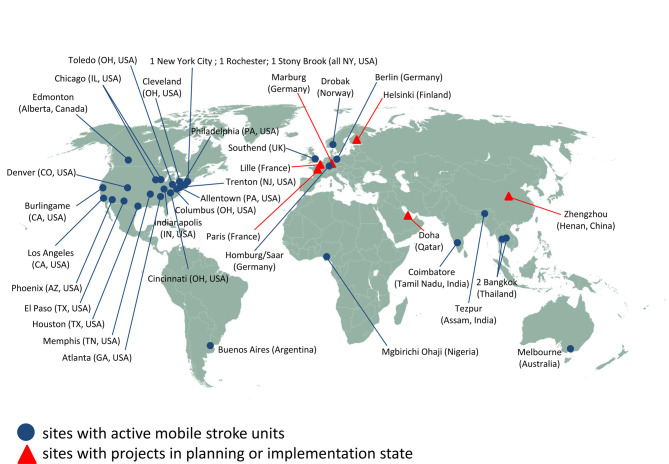
Since its first introduction in clinical practice in 2008, the concept of mobile stroke unit enabling prehospital stroke treatment has rapidly expanded worldwide. This review summarises current knowledge in this young field of stroke research, discussing topics such as benefits in reduction of delay before treatment, vascular imaging-based triage of patients with large-vessel occlusion in the field, differential blood pressure management or prehospital antagonisation of anticoagulants. However, before mobile stroke units can become routine, several questions remain to be answered. Current research, therefore, focuses on safety, long-term medical benefit, best setting and cost-efficiency as crucial determinants for the sustainability of this novel strategy of acute stroke management.
Keywords: stroke.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources