

Cost-effectiveness of a hypothetical cell or gene therapy cure for sickle cell disease
- PMID: 34035408
- PMCID: PMC8149675
- DOI: 10.1038/s41598-021-90405-1
Cost-effectiveness of a hypothetical cell or gene therapy cure for sickle cell disease
Abstract
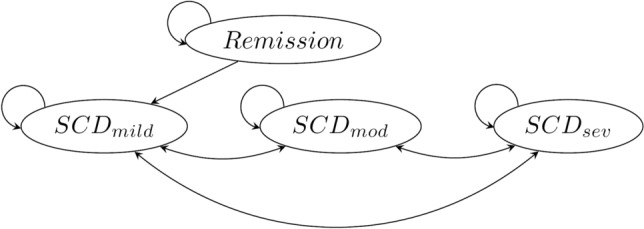
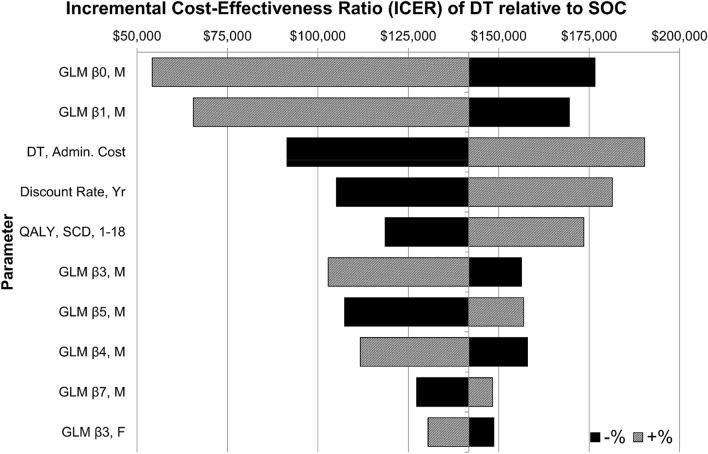
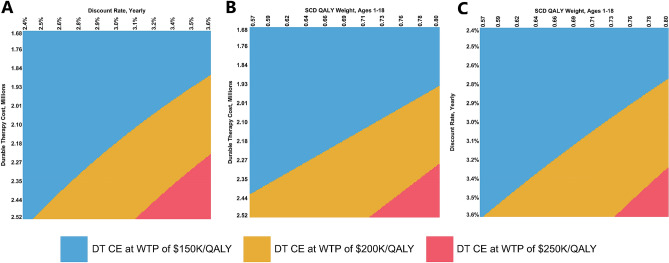
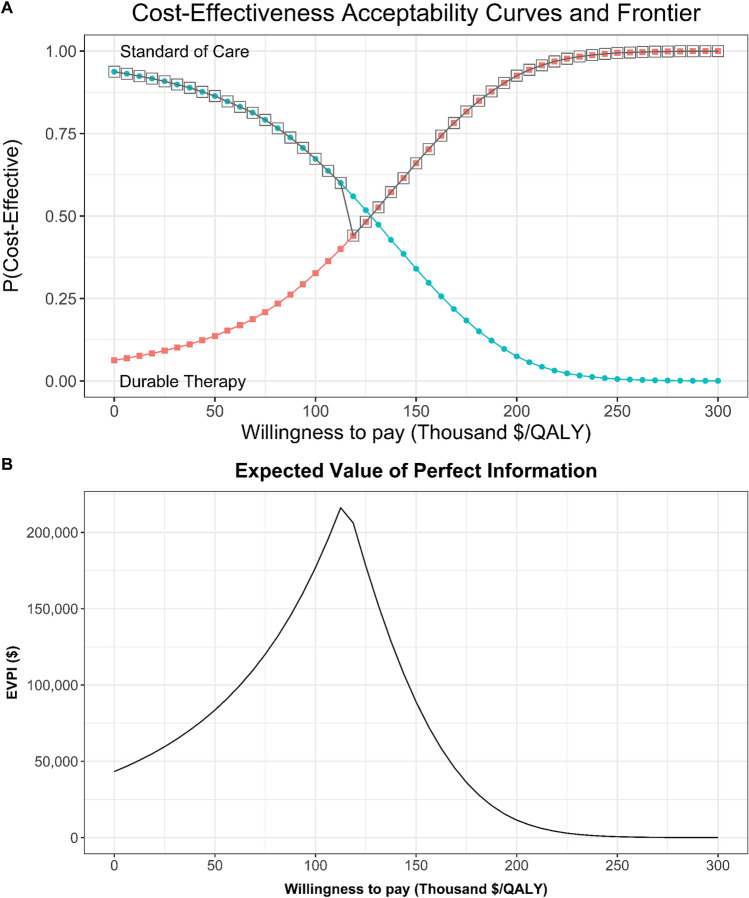
Sickle cell disease (SCD) is a group of inherited genetic conditions associated with lifelong complications and increased healthcare resource utilization. Standard treatment for SCD in the US varies based on stage of the disease and observed clinical severity. In this study, we aim to evaluate the potential cost-effectiveness of a durable cell or gene therapy cure for sickle cell disease from the US healthcare sector perspective. We developed a lifetime Markov model to evaluate the cost-effectiveness of a hypothetical single-administration durable treatment (DT) for SCD provided at birth, relative to standard of care (SOC). We informed model inputs including direct healthcare costs, health state utility weights, transition probabilities, and mortality rates using a retrospective database analysis of commercially insured individuals and the medical literature. Our primary outcome of interest was the incremental cost-effectiveness ratio (ICER) of DT versus SOC evaluated at a base case willingness-to-pay (WTP) threshold of $150,000 per quality-adjusted life year (QALY). We tested the robustness of our base case findings through scenario, deterministic sensitivity (DSA), and probabilistic sensitivity analyses (PSA). In the base case analysis, treatment with DT was cost-effective with an ICER of $140,877/QALY relative to SOC for a hypothetical cohort involving 47% females. Both males (ICER of $135,574/QALY) and females (ICER of $146,511/QALY) were similarly cost-effective to treat. In univariate DSA the base case ICER was most sensitive to the costs of treating males, DT treatment cost, and the discount rate. In PSA, DT was cost-effective in 32.7%, 66.0%, and 92.6% of 10,000 simulations at WTP values of $100,000, $150,000, and $200,000 per QALY, respectively. A scenario analysis showed cost-effectiveness of DT is highly contingent on assumed lifetime durability of the cure. A hypothetical cell or gene therapy cure for SCD is likely to be cost-effective from the US healthcare sector perspective. Large upfront costs of a single administration cure are offset by significant downstream gains in health for patients treated early in life. We find cost-effectiveness outcomes do not vary substantially by gender; however, several model parameters including assumed durability and upfront cost of DT are likely to influence cost-effectiveness findings.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- National Heart, Lung & and Blood Institute . Evidence-Based Management of Sickle Cell Disease: Expert Panel report, 2014. National Institutes of Health; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
