

Acute and long-term disruption of glycometabolic control after SARS-CoV-2 infection
- PMID: 34035524
- PMCID: PMC9931026
- DOI: 10.1038/s42255-021-00407-6
Acute and long-term disruption of glycometabolic control after SARS-CoV-2 infection
Abstract
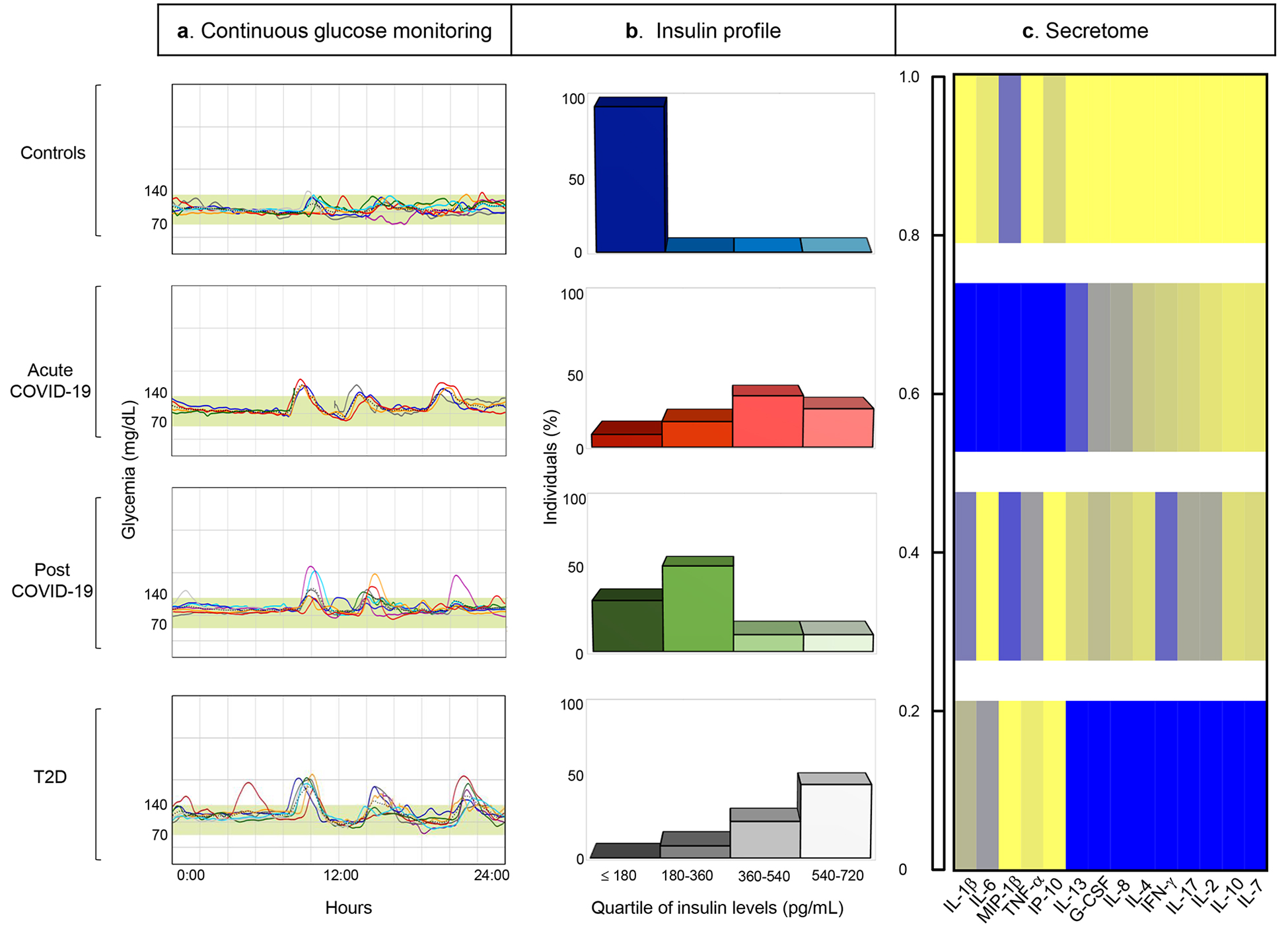
Patients with coronavirus disease 2019 (COVID-19) are reported to have a greater prevalence of hyperglycaemia. Cytokine release as a consequence of severe acute respiratory syndrome coronavirus 2 infection may precipitate the onset of metabolic alterations by affecting glucose homeostasis. Here we describe abnormalities in glycometabolic control, insulin resistance and beta cell function in patients with COVID-19 without any pre-existing history or diagnosis of diabetes, and document glycaemic abnormalities in recovered patients 2 months after onset of disease. In a cohort of 551 patients hospitalized for COVID-19 in Italy, we found that 46% of patients were hyperglycaemic, whereas 27% were normoglycaemic. Using clinical assays and continuous glucose monitoring in a subset of patients, we detected altered glycometabolic control, with insulin resistance and an abnormal cytokine profile, even in normoglycaemic patients. Glycaemic abnormalities can be detected for at least 2 months in patients who recovered from COVID-19. Our data demonstrate that COVID-19 is associated with aberrant glycometabolic control, which can persist even after recovery, suggesting that further investigation of metabolic abnormalities in the context of long COVID is warranted.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures




Comment in
-
How COVID-19 disrupts glycometabolic control.Nat Rev Endocrinol. 2021 Aug;17(8):448. doi: 10.1038/s41574-021-00526-w. Nat Rev Endocrinol. 2021. PMID: 34127837 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
