

Epidemiologic Trends and Diagnostic Evaluation of Fecal Incontinence
- PMID: 34035733
- PMCID: PMC8132710
Epidemiologic Trends and Diagnostic Evaluation of Fecal Incontinence
Abstract
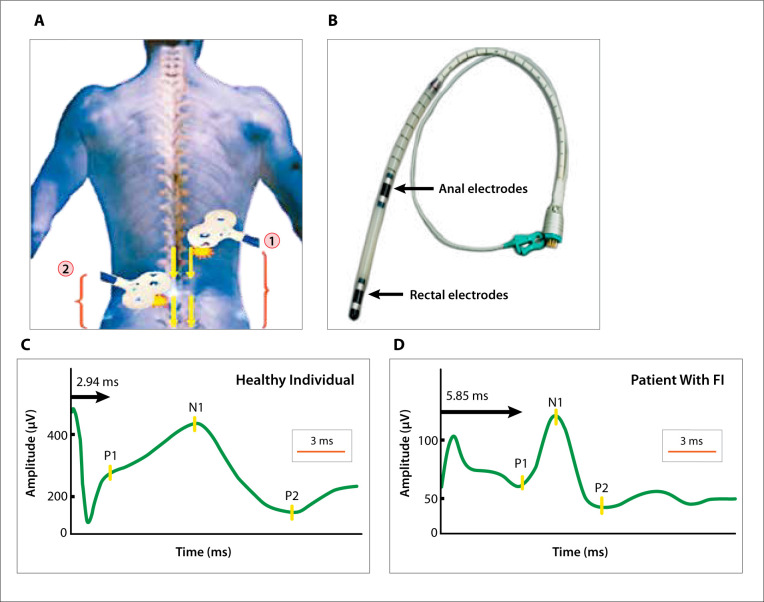
Fecal incontinence (FI) is a prevalent condition that occurs in up to 15% of the Western population and significantly impairs quality of life. The current understanding of the epidemiology of FI is shifting because of an increasing recognition of FI in men, better appreciation for the impact of changing obstetric practices on FI in women, and comprehension of the effect of modifiable risk factors on the development of FI over time. The pathophysiology of FI is complex and multifactorial, which necessitates the use of multiple diagnostic tests, including tests of anorectal sensorimotor function, peripheral nerve function, and anatomic structure. Translumbosacral anorectal magnetic stimulation is an emerging noninvasive diagnostic test for assessing lumbosacral neuropathy. This article is not intended as a comprehensive recitation of the literature, but rather focuses on recent developments in the understanding of the epidemiology of FI, as well as on the diagnostic evaluation of this condition. This article aims to increase awareness of FI and to outline an initial diagnostic approach to affected patients.
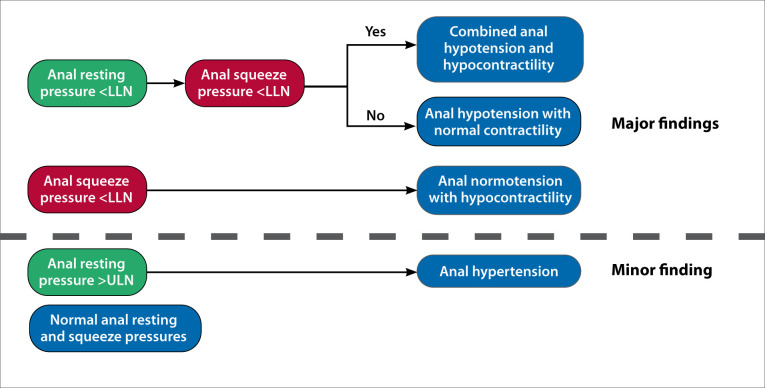
Keywords: Fecal incontinence; International Anorectal Physiology Working Group; London classification; high-resolution anorectal manometry; translumbosacral anorectal magnetic stimulation.
Copyright © 2020, Gastro-Hep Communications, Inc.
Conflict of interest statement
Dr Sharma has no relevant conflicts of interest to disclose. Dr Rao serves on the advisory board for, and has received stock options from, InTone MV.
Figures
Similar articles
-
Effects of Translumbosacral Neuromodulation Therapy on Gut and Brain Interactions and Anorectal Neuropathy in Fecal Incontinence: A Randomized Study.Neuromodulation. 2021 Oct;24(7):1269-1277. doi: 10.1111/ner.13485. Epub 2021 Jun 22. Neuromodulation. 2021. PMID: 34156730 Free PMC article. Clinical Trial.
-
Translumbosacral Neuromodulation Therapy for Fecal Incontinence: A Randomized Frequency Response Trial.Am J Gastroenterol. 2021 Jan 1;116(1):162-170. doi: 10.14309/ajg.0000000000000766. Am J Gastroenterol. 2021. PMID: 32740081 Free PMC article.
-
The relationships between the results of contemporary tests of anorectal structure and sensorimotor function and the severity of fecal incontinence.Neurogastroenterol Motil. 2020 Nov;32(11):e13946. doi: 10.1111/nmo.13946. Epub 2020 Jul 19. Neurogastroenterol Motil. 2020. PMID: 32683767
-
Assessing Anorectal Function in Constipation and Fecal Incontinence.Gastroenterol Clin North Am. 2020 Sep;49(3):589-606. doi: 10.1016/j.gtc.2020.04.011. Epub 2020 Jun 20. Gastroenterol Clin North Am. 2020. PMID: 32718572 Review.
-
Diagnostic approach to faecal incontinence: What test and when to perform?World J Gastroenterol. 2021 Apr 21;27(15):1553-1562. doi: 10.3748/wjg.v27.i15.1553. World J Gastroenterol. 2021. PMID: 33958842 Free PMC article. Review.
Cited by
-
Role of Hypoxic Secretome from Mesenchymal Stem Cells in Enhancing Tissue Repair: Regulatory Effects on HIF-1α, VEGF, and Fibroblast in a Sphincterotomy Rat Model.J Inflamm Res. 2024 Oct 21;17:7463-7484. doi: 10.2147/JIR.S480061. eCollection 2024. J Inflamm Res. 2024. PMID: 39464333 Free PMC article.
-
Electroceuticals and Magnetoceuticals in Gastroenterology.Biomolecules. 2024 Jun 26;14(7):760. doi: 10.3390/biom14070760. Biomolecules. 2024. PMID: 39062474 Free PMC article. Review.
-
Clinical Evaluation of a Patient With Symptoms of Colonic or Anorectal Motility Disorders.J Neurogastroenterol Motil. 2020 Sep 30;26(4):423-436. doi: 10.5056/jnm20012. J Neurogastroenterol Motil. 2020. PMID: 32989182 Free PMC article. Review.
References
-
- Whitehead WE, Simren M, Busby-Whitehead J et al. Fecal incontinence diagnosed by the Rome IV criteria in the United States, Canada, and the United Kingdom. Clin Gastroenterol Hepatol. 2020;18(2):385–391. - PubMed
-
- Whitehead WE, Rao SS, Lowry A et al. Treatment of fecal incontinence: state of the science summary for the National Institute of Diabetes and Digestive and Kidney Diseases workshop. Am J Gastroenterol. 2015;110(1):138–146. - PubMed
LinkOut - more resources
Full Text Sources