

Improving osteoporotic vertebral deformity detection on chest frontal view radiograph by adjusted X-ray beam positioning
- PMID: 34036040
- PMCID: PMC8121774
- DOI: 10.1016/j.jot.2021.04.001
Improving osteoporotic vertebral deformity detection on chest frontal view radiograph by adjusted X-ray beam positioning
Abstract
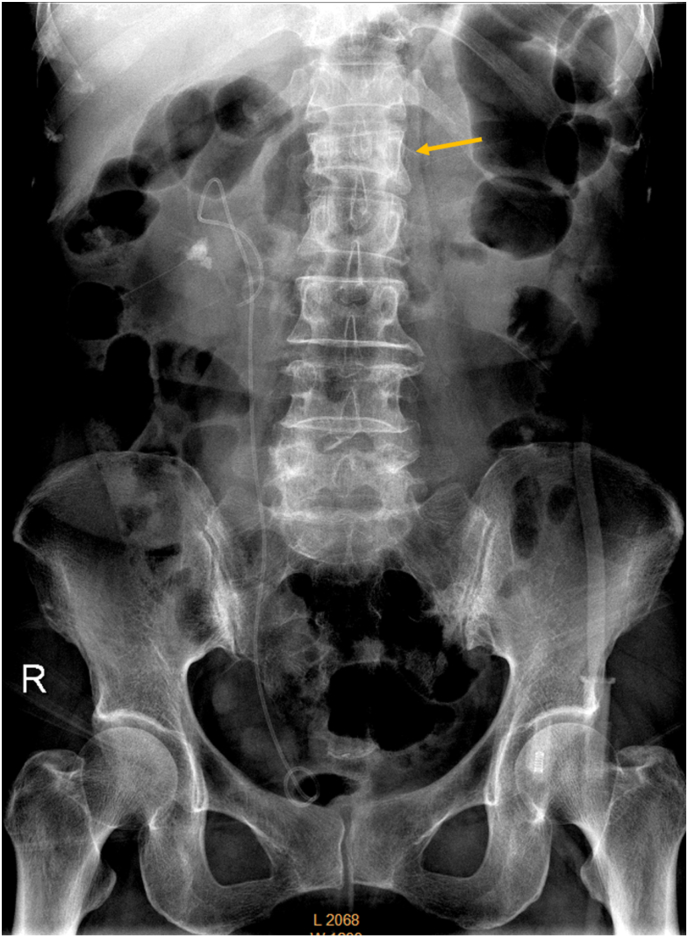
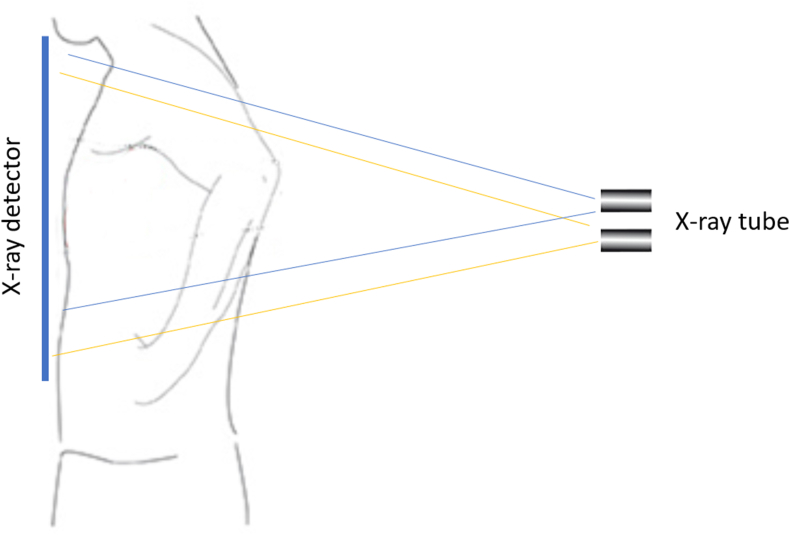
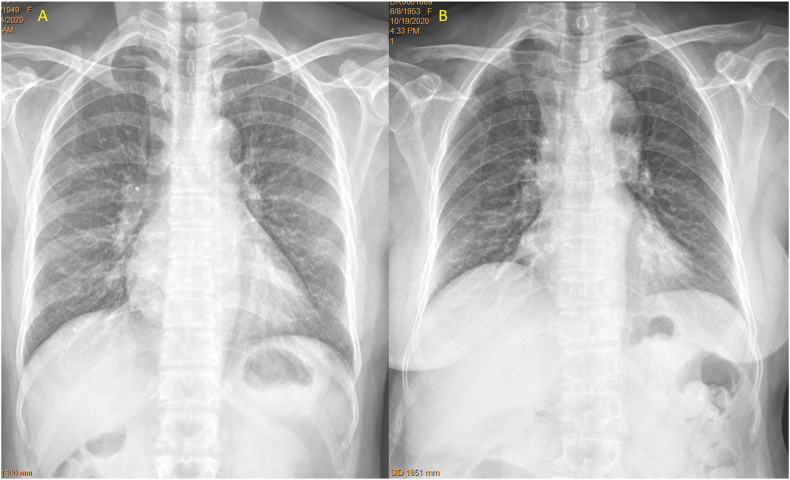
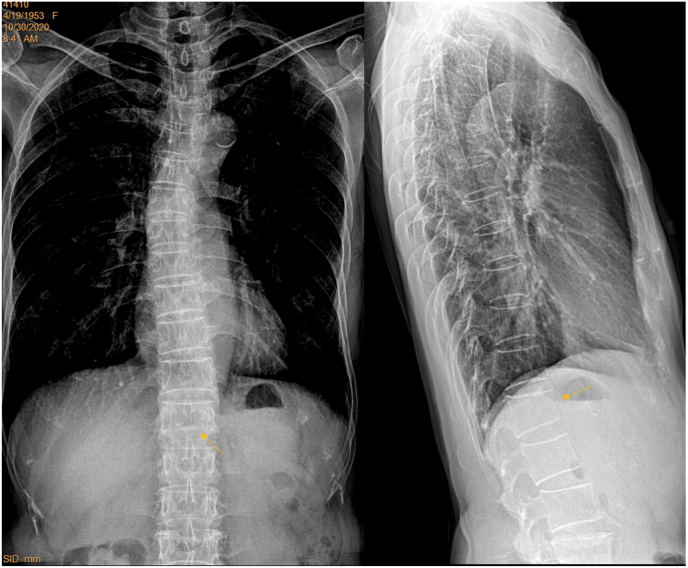
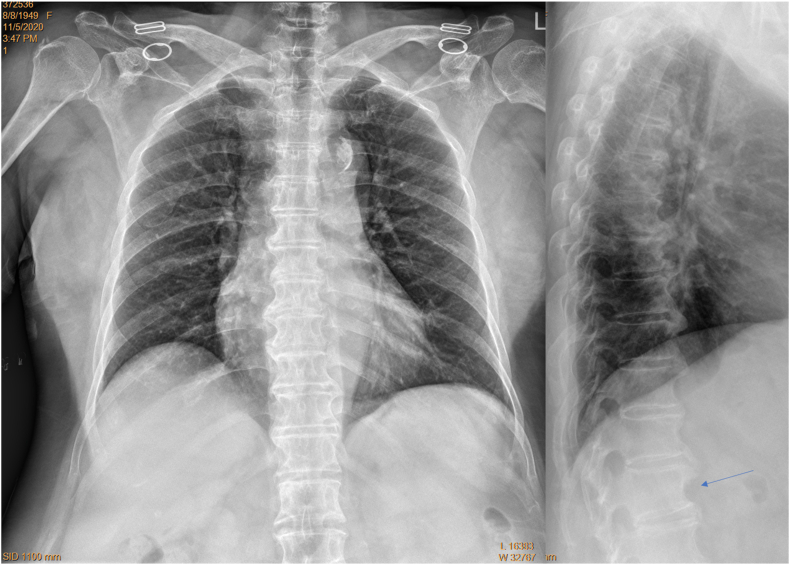
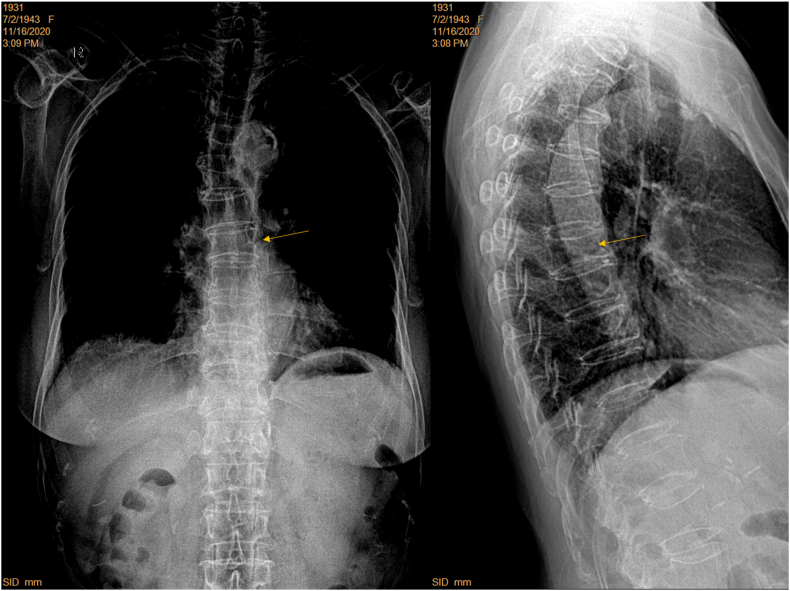
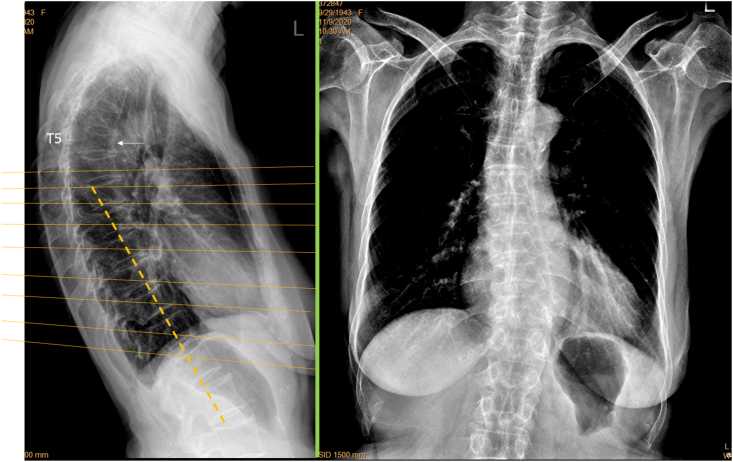
Purpose: In clinics, chest frontal view radiograph (CFR) is often taken for patients suspected of respiratory diseases and for assessing the heart and big vessels. CFR can be utilised to opportunistically detect osteoporotic vertebral fracture (OVF). However, for standard CFR, the site of highest OVF prevalence, i.e., the thoracolumbar junction, is usually 'off-centre' to the X-ray beam focus. This study tested the hypothesis that, if a CRF is taken with approximately two vertebrae lower than the standard X-ray beam positioning, the visualization of thoraco-lumbar junction can be much improved.
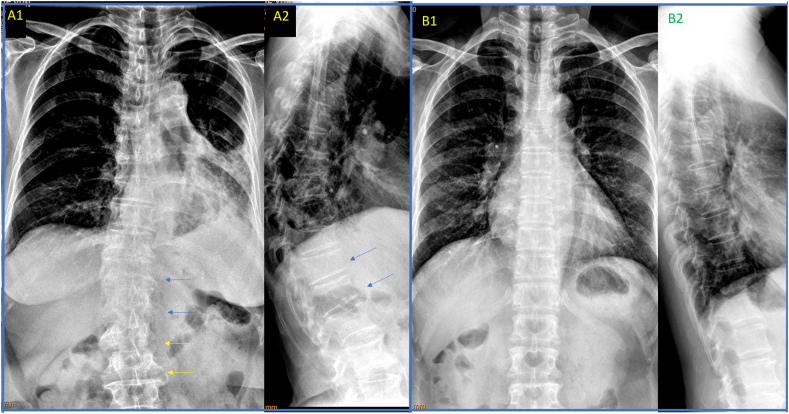
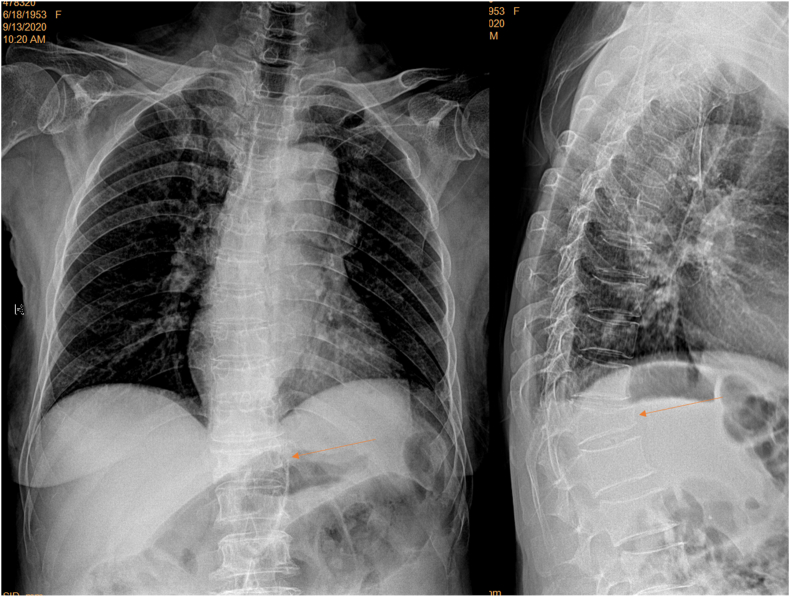
Materials: Four hospitals (A, B, C, D) provided 101 elderly women's digital CFRs with standard filming (28, 20, 24, and 21 cases respectively). Eighty four elderly female patients were prospectively recruited from hospitals-A and B, who were consecutive patients referred for chest radiograph with indications other than spine disorders. For theses prospective CFRs, the focus of X-ray beam was adjusted from towards vertebra T6 to towards T8, and standard lateral radiographs were obtained for reference. Visibility of spine and detectability of OVF were assessed on the CFRs. OVF was diagnosed based on chest lateral radiograph (CLR) after excluding other potential causes both radiographically and clinically.
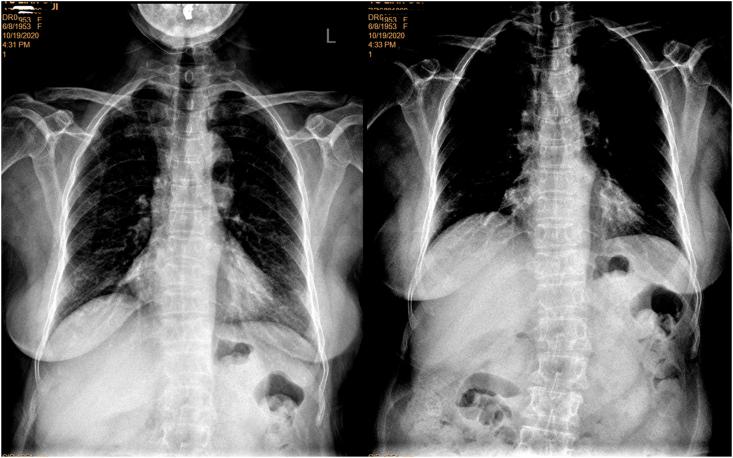
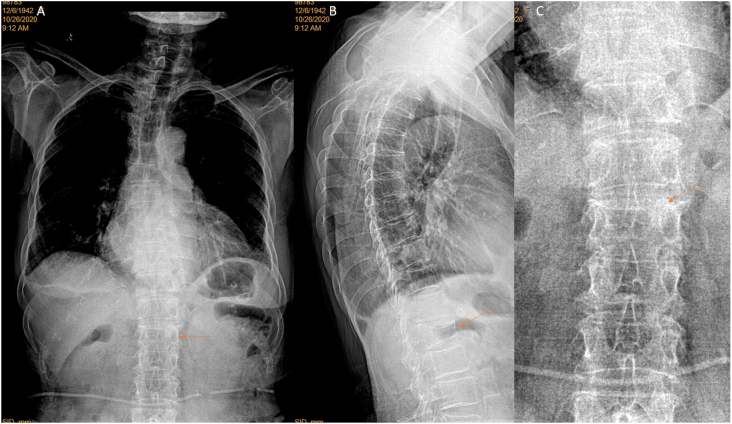
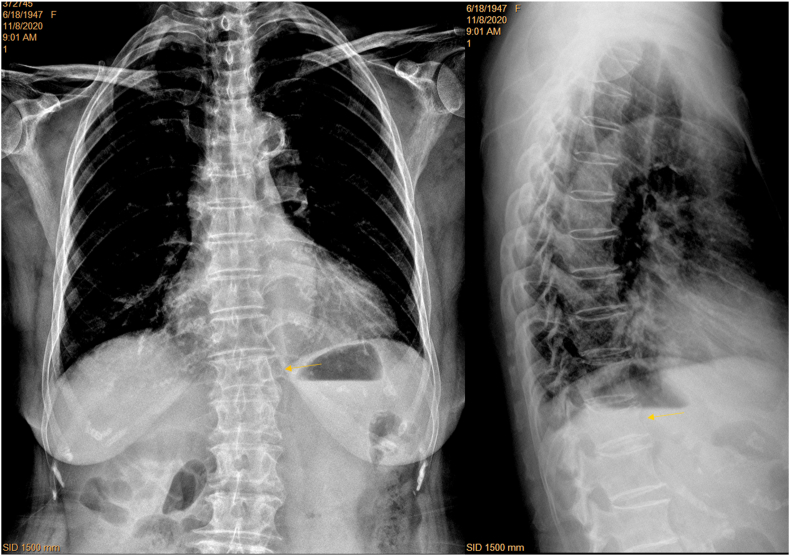
Results: For standardly filmed CFR, spine readability was similar among those from Hospitals-A, B, and C, while performed less well for those from Hospital-D. With the prospective cases from Hospitals-A and B, spines readable to vertebra L1 level or lower increased from 48.2% for standard filming to 80.7% for adjusted filming. Spines with 'blurry' labelling decreased from 35.7% for standard filming to 15.7% for adjusted filming. For the 84 prospective cases, 42.9% (36/84) of the patients had OVF, and 26 cases of CLR positive cases were detected as having vertebral deformity on CFR. For minimal OVF cases (<20% height loss), 38% (5/13) were detected on CFR. Among 22 cases with apparent OVF (≥20% height loss), two cases were missed on CFR. False positivity was labelled in five cases, among them four cases had 'burry' spines.
Conclusion: CFR can help opportunistically detect OVF, which can be further improved if X-ray beam is adjusted to towards vertebra T8 instead of towards vertebra T6.
The translational potential of this article: This study confirms that CFR can help detect OVF opportunistically, and the visibility of the mid/lower thoracic spine and thoracolumbar junction can be much improved after minor adjustment of X-ray beam positioning. This study also suggests high positive rate of OVF in elderly Chinese female patients indicated for chest radiograph. Radiologists should be trained and sensitized in vertebral deformity identification on CFR as the clinical management can be improved by opportunistic detection of OVF.
Keywords: Chest; Frontal view; Osteoporosis; Radiograph; Vertebral deformity; Vertebral fracture.
© 2021 The Authors.
Conflict of interest statement
Authors Er-Zhu Du, Wei-Hong Liu, and Yì Xiáng Wáng all declare no conflict of interest.
Figures

Similar articles
-
A software program for automated compressive vertebral fracture detection on elderly women's lateral chest radiograph: Ofeye 1.0.Quant Imaging Med Surg. 2022 Aug;12(8):4259-4271. doi: 10.21037/qims-22-433. Quant Imaging Med Surg. 2022. PMID: 35919046 Free PMC article.
-
CT detects more osteoporotic endplate depressions than radiograph: a descriptive comparison of 76 vertebrae.Osteoporos Int. 2022 Jul;33(7):1569-1577. doi: 10.1007/s00198-022-06391-1. Epub 2022 Apr 4. Osteoporos Int. 2022. PMID: 35368223
-
Interpretation of osteoporotic vertebral deformity on frontal view radiographs of the chest and abdomen: a pictorial review.Quant Imaging Med Surg. 2021 Jan;11(1):423-442. doi: 10.21037/qims-2020-28. Quant Imaging Med Surg. 2021. PMID: 33392042 Free PMC article. Review.
-
Radiological diagnosis of prevalent osteoporotic vertebral fracture on radiographs: an interim consensus from a group of experts of the ESSR osteoporosis and metabolism subcommittee.Skeletal Radiol. 2024 Dec;53(12):2563-2574. doi: 10.1007/s00256-024-04678-4. Epub 2024 Apr 25. Skeletal Radiol. 2024. PMID: 38662094 Free PMC article. Review.
-
Recognizing osteoporotic vertebral deformity on frontal view radiograph: a cohort analysis and a pictorial review.Arch Osteoporos. 2020 Mar 6;15(1):41. doi: 10.1007/s11657-020-00716-5. Arch Osteoporos. 2020. PMID: 32144508
Cited by
-
'Healthier Chinese spine': an update of osteoporotic fractures in men (MrOS) and in women (MsOS) Hong Kong spine radiograph studies.Quant Imaging Med Surg. 2022 Mar;12(3):2090-2105. doi: 10.21037/qims-2021-07. Quant Imaging Med Surg. 2022. PMID: 35284274 Free PMC article. Review.
-
Vertebral fracture severity assessment on anteroposterior radiographs with a new semi-quantitative technique.Osteoporos Int. 2024 May;35(5):831-839. doi: 10.1007/s00198-024-07024-5. Epub 2024 Jan 31. Osteoporos Int. 2024. PMID: 38296865
-
An update of our understanding of radiographic diagnostics for prevalent osteoporotic vertebral fracture in elderly women.Quant Imaging Med Surg. 2022 Jul;12(7):3495-3514. doi: 10.21037/qims-22-360. Quant Imaging Med Surg. 2022. PMID: 35782246 Free PMC article. No abstract available.
References
-
- Kim D.H., Vaccaro A.R. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006;6:479–487. - PubMed
-
- Delmas P.D., van de Langerijt L., Watts N.B., Eastell R., Genant H., Grauer A. IMPACT Study Group. Underdiagnosis of vertebral fractures is a worldwide problem: the IMPACT study. J Bone Miner Res. 2005;20:557–563. - PubMed
-
- Diacinti D., Vitali C., Gussoni G., Pisani D., Sinigaglia L., Bianchi G. Research Department of FADOI. Misdiagnosis of vertebral fractures on local radiographic readings of the multicentre POINT (prevalence of osteoporosis in INTernal medicine) study. Bone. 2017;101:230–235. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
