

Cardiovascular adverse events in pregnancy: A global perspective
- PMID: 34036091
- PMCID: PMC8133785
- DOI: 10.21542/gcsp.2021.5
Cardiovascular adverse events in pregnancy: A global perspective
Abstract
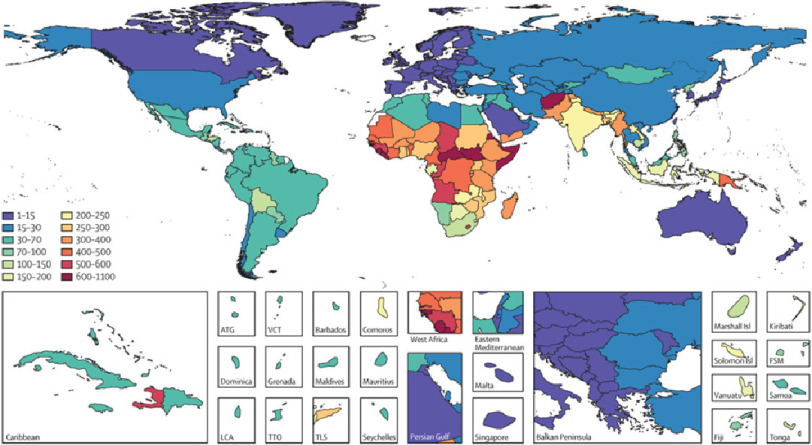
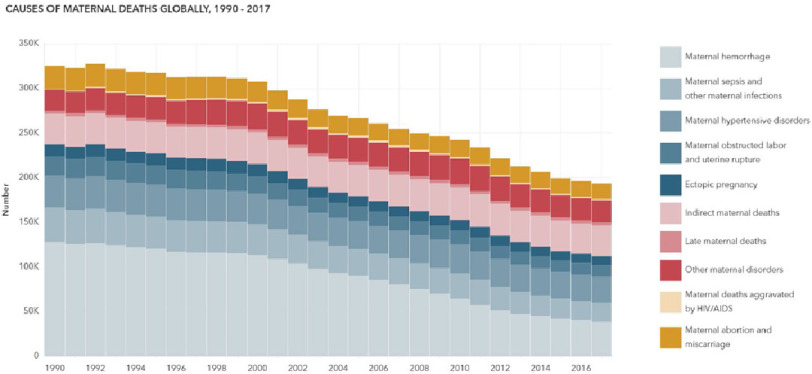
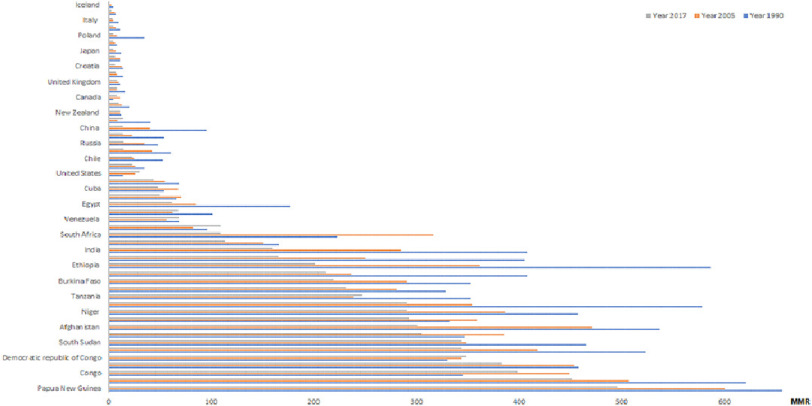
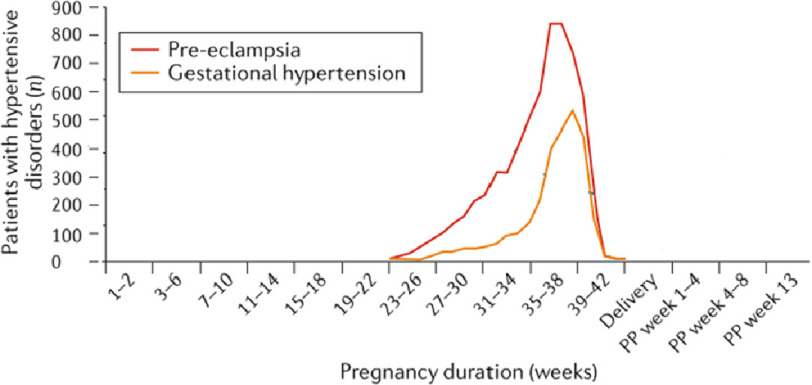
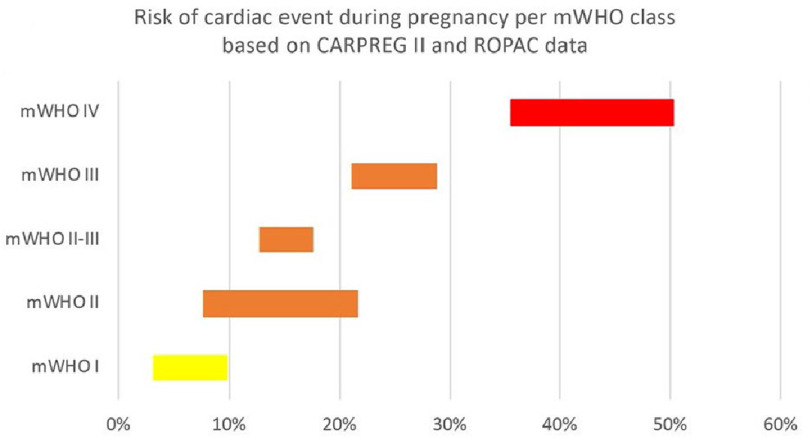
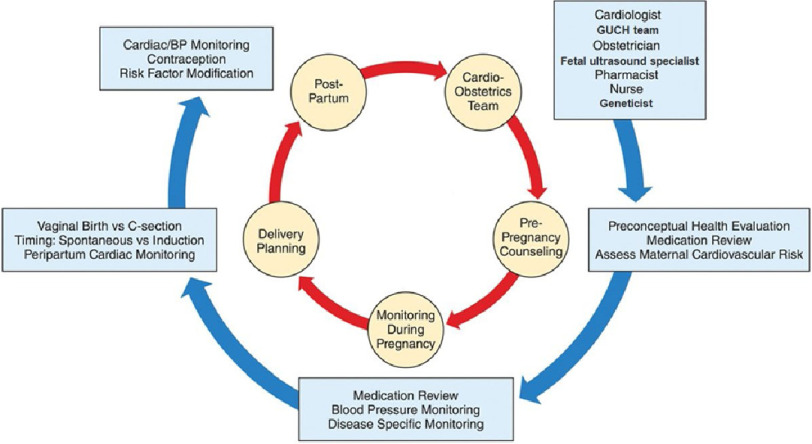
Pregnant women with heart disease are vulnerable to many adverse cardiovascular events (AE). AEs during and after pregnancy continue to be important causes of maternal mortality and morbidity worldwide, with huge variations in burden in different countries and regions. These AEs are classified as having direct or indirect causes, depending on whether they are directly caused by pregnancy or due to some pre-existing disease and/or non-obstetric cause, respectively. The risks continue throughout pregnancy and even after childbirth. Apart from immediate complications during pregnancy, there is increasing evidence of a significant link between several events and the risk of cardiovascular disease (CVD) later in life. A significant number of pregnancy-related deaths caused by cardiovascular disease are preventable. This prevention can be realized through increasing awareness of cardiovascular AE in pregnancy, coupled with the application of strategies for prevention and treatment. Knowledge of the risks associated with CVD and pregnancy is of extreme importance in that regard. We discuss the global distribution of cardiovascular maternal mortality, adverse events during and after pregnancy, their predictors and risk stratification. In addition, we enumerate possible solutions, particularly the role of cardio-obstetric clinics.
Copyright ©2021 The Author(s).
Figures
References
-
- IHME . Inst Heal Metrics Eval (IHME) Seattle. WA IHME; 2018. Findings from the Global Burden of Disease Study 2017 (GBD 2017)
-
- Maternal Health Atlas [4 December 2020]. https://maternalhealthatlas.org/
-
- 2012. [13 January 2021]. The WHO Application of ICD-10 to Deaths during Pregnancy, Childbirth and the Puerperium: ICD-MM. http://www.who.int/about/licensing/
Publication types
LinkOut - more resources
Full Text Sources