

NTRK Fusions Identified in Pediatric Tumors: The Frequency, Fusion Partners, and Clinical Outcome
- PMID: 34036219
- PMCID: PMC8140782
- DOI: 10.1200/PO.20.00250
NTRK Fusions Identified in Pediatric Tumors: The Frequency, Fusion Partners, and Clinical Outcome
Abstract
Purpose: Neurotrophic tyrosine receptor kinase (NTRK) fusions have been described as oncogenic drivers in a variety of tumors. However, little is known about the overall frequency of NTRK fusion in unselected pediatric tumors. Here, we assessed the frequency, fusion partners, and clinical course in pediatric patients with NTRK fusion-positive tumors.
Patients and methods: We studied 1,347 consecutive pediatric tumors from 1,217 patients who underwent tumor genomic profiling using custom-designed DNA and RNA next-generation sequencing panels. NTRK fusions identified were orthogonally confirmed.
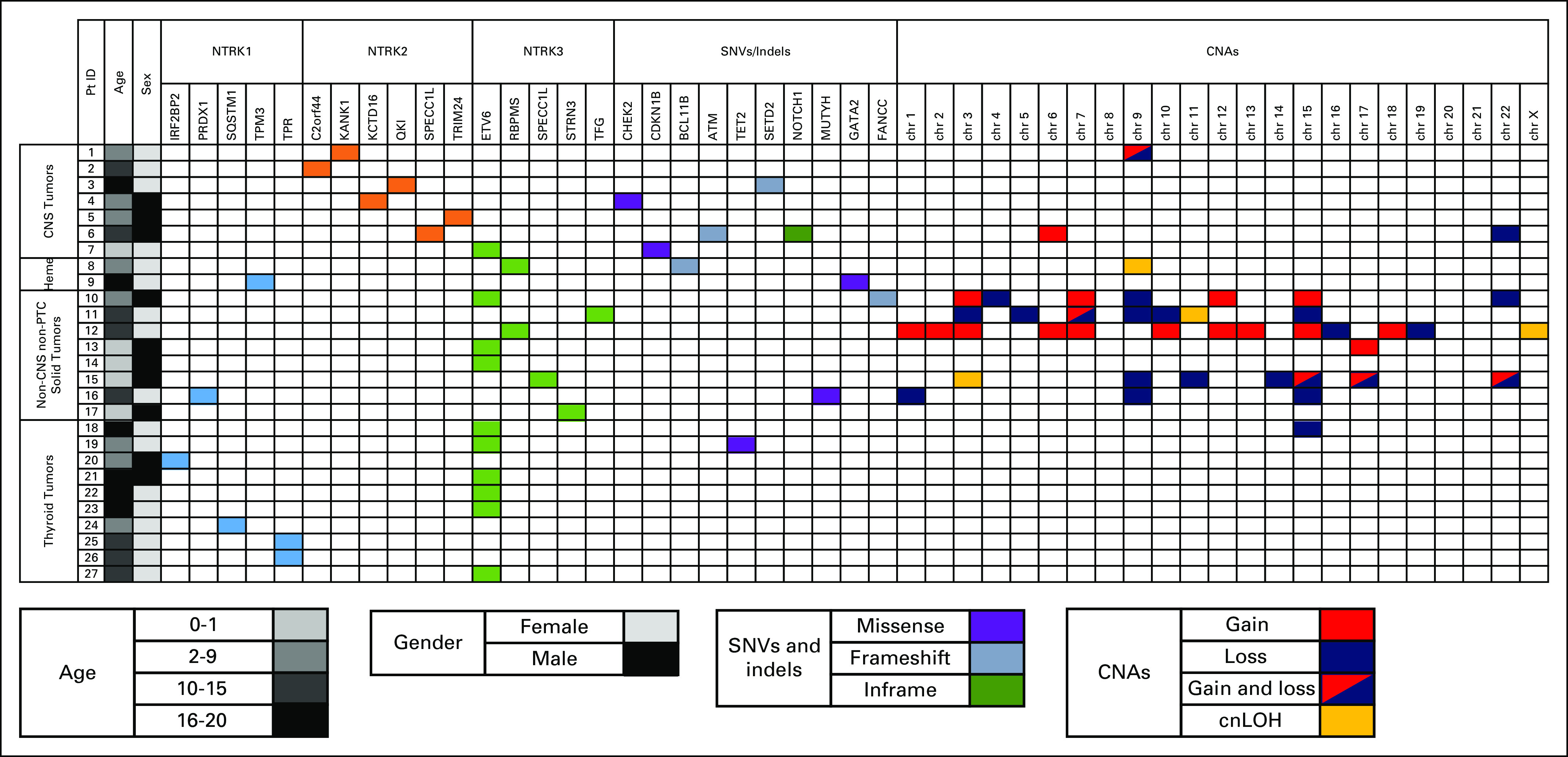
Results and discussion: NTRK fusions were identified in 29 tumors from 27 patients with a positive yield of 2.22% for all patients and 3.08% for solid tumors. Although NTRK2 fusions were found exclusively in CNS tumors and NTRK1 fusions were highly enriched in papillary thyroid carcinomas, NTRK3 fusions were identified in all tumor categories. The most canonical fusion was ETV6-NTRK3 observed in 10 patients with diverse types of tumors. Several novel NTRK fusions were observed in rare tumor types, including KCTD16-NTRK1 in ganglioglioma and IRF2BP2-NTRK3 in papillary thyroid carcinomas. The detection of an NTRK fusion confirmed the morphologic diagnosis including five cases where the final tumor diagnosis was largely based on the discovery of an NTRK fusion. In one patient, the diagnosis was changed because of the identification of an ETV6-NTRK3 fusion. One patient with infantile fibrosarcoma was treated with larotrectinib and achieved complete pathologic remission.
Conclusion: NTRK fusions are more frequently seen in pediatric tumors than in adult tumors and involve a broader panel of fusion partners and a wider range of tumors than previously recognized. These results highlight the importance of screening for NTRK fusions as part of the tumor genomic profiling for patients with pediatric cancer.
© 2021 by American Society of Clinical Oncology.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/cci/author-center. Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments). Elizabeth FoxOther Relationship: Helsinn TherapeuticsGerald B. WertheimEmployment: Johnson & Johnson Stock and Other Ownership Interests: Johnson & JohnsonVinodh PillaiConsulting or Advisory Role: Foundation medicine Travel, Accommodations, Expenses: Foundation MedicineJennifer E. PogorilerEmployment: Bristol-Myers Squibb Stock and Other Ownership Interests: Bristol-Myers SquibbStephen P. HungerStock and Other Ownership Interests: Amgen, Merck Honoraria: Amgen Consulting or Advisory Role: NovartisAndrew J. BauerHonoraria: Sandoz-Novartis Travel, Accommodations, Expenses: SandozMarilyn M. LiConsulting or Advisory Role: Roche No other potential conflicts of interest were reported
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
