

Surveillance for Outcomes Selected as Atrial Fibrillation Quality Indicators in Canada: 10-Year Trends in Stroke, Major Bleeding, and Heart Failure
- PMID: 34036258
- PMCID: PMC8134946
- DOI: 10.1016/j.cjco.2021.01.003
Surveillance for Outcomes Selected as Atrial Fibrillation Quality Indicators in Canada: 10-Year Trends in Stroke, Major Bleeding, and Heart Failure
Abstract
Background: Whether advances in identification and management of atrial fibrillation and atrial flutter (collectively, AF) have led to improved outcomes is unclear. We sought to study trends in clinical outcomes selected as quality indicators for nonvalvular AF in Canada.
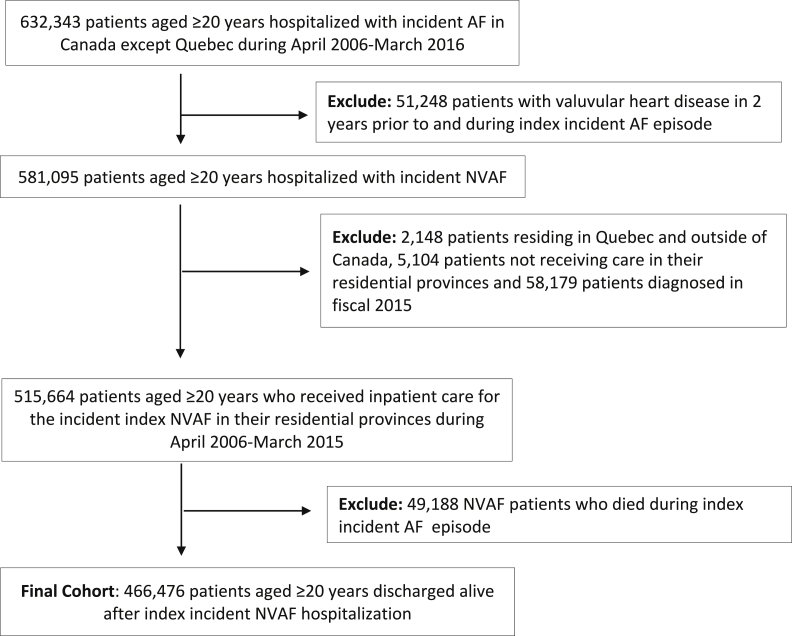
Methods: We identified hospitalized patients with a first diagnosis of nonvalvular AF between April 2006 and March 2015, in all of Canada except Quebec. We assessed trends in 1-year incidence of stroke/systemic embolism (SSE), major bleeding, and initial heart failure (HF) hospitalization.
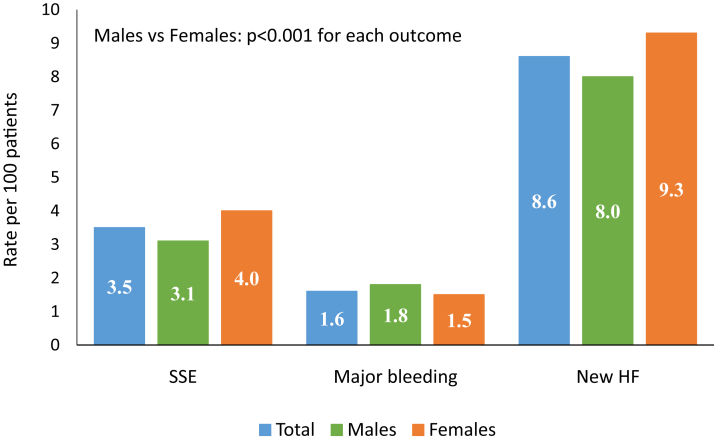
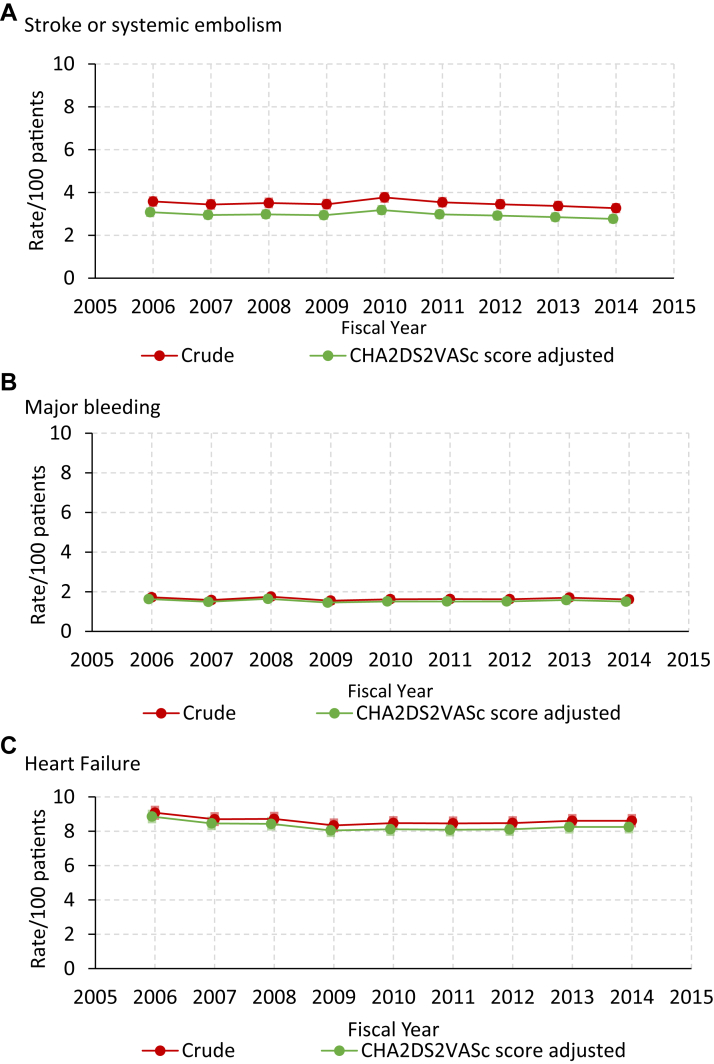
Results: The cohort included 466,476 patients. The median age was 77 years (interquartile range, 68-84 years), 46% were female, and 68% had a Congestive Heart Failure, Hypertension, Age (≥75 years), Diabetes, Stroke/Transient Ischemic Attack, Vascular Disease, Age (65-74 years), Sex (Female) (CHA2DS2-VASc) score > 3. Within 1 year of discharge, 3.5% were hospitalized for stroke or SSE, 1.6% for major bleeding, and 8.6% for new HF. Over the study period, the crude rate of SSE declined from 3.6% to 3.3% (P = 0.002), whereas the rates of hospitalization for new HF and for major bleeding did not significantly change. After adjustment for CHA2DS2-VASc score, the yearly rates of incident SSE (risk ratio, 0.99; 95% confidence interval [CI], 0.98-0.99; P = 0.002) and HF (risk ratio, 0.99; 95% CI, 0.99-1.00; P = 0.001) declined ≤ 1% absolute, whereas major bleeding remained unchanged (risk ratio, 1.00; 95% CI, 0.99-1.00; P = 0.28).
Conclusions: Among hospitalized patients with nonvalvular AF in Canada, the rate of SSE and new HF decreased modestly over a 10-year period, with no significant change in major bleeding. Efforts to study process-based quality indicators, with increased focus on HF prevention, are needed.
Contexte: On ne sait pas si les avancées en matière de détection et de prise en charge de la fibrillation auriculaire et du flutter auriculaire (collectivement appelés « FA » ci-après) ont permis d’améliorer les résultats pour les patients. Nous avons donc étudié les tendances à l’égard de résultats cliniques particuliers pris comme indicateurs de qualité relatifs à la FA non valvulaire au Canada.
Méthodologie: Nous avons recensé les patients hospitalisés au Canada (sauf au Québec) entre avril 2006 et mars 2015 en raison d’une FA non valvulaire nouvellement diagnostiquée. Nous avons évalué les tendances quant à la survenue d’un accident vasculaire cérébral ou d’une embolie systémique (AVC/ES), d’une hémorragie majeure et d’une première hospitalisation pour insuffisance cardiaque.
Résultats: La cohorte comprenait 466 476 patients, dont l’âge médian était de 77 ans (intervalle interquartile : 68 à 84 ans); 46 % des patients étaient des femmes, et 68 % avaient un score CHA2DS2-VASc ( C ongestive Heart Failure [insuffisance cardiaque congestive], hypertension, âge [≥ 75 ans], diabète, S troke/Transient Ischemic Attack [AVC/accident ischémique transitoire] – maladie vasculaire, âge [65-74 ans], sexe [femmes]) supérieur à 3. Dans l’année suivant la sortie de l’hôpital, 3,5 % des patients ont été hospitalisés en raison d’un AVC ou d’un AVC/ES, 1,6 %, en raison d’une hémorragie majeure et 8,6 %, en raison d’une nouvelle insuffisance cardiaque. Au cours de la période étudiée, le taux brut d’AVC/ES est passé de 3,6 % à 3,3 % (p = 0,002), tandis que les taux d’hospitalisation en raison d’une nouvelle insuffisance cardiaque ou d’une hémorragie majeure n’ont pas changé de manière significative. Après correction pour tenir compte du score CHA2DS2-VASc, les taux annuels de survenue d’un AVC/ES (rapport des risques de 0,99; intervalle de confiance [IC] à 95 % : de 0,98 à 0,99; p = 0,002) et d’une insuffisance cardiaque (rapport des risques de 0,99; IC à 95 % : de 0,99 à 1,00; p = 0,001) ont diminué de ≤ 1 % en valeur absolue, tandis que le taux de survenue d’une hémorragie majeure n’a pas changé (rapport des risques : 1,00; IC à 95 % : de 0,99 à 1,00; p = 0,28).
Conclusions: Parmi les patients hospitalisés au Canada en raison d’une FA non valvulaire, les taux d’AVC/ES et de nouvelle insuffisance cardiaque ont affiché une réduction modeste sur une période de 10 ans, tandis que le taux d’hémorragie majeure n’a pas changé de manière significative. D’autres études évaluant les indicateurs de qualité fondés sur les procédés, notamment en matière de prévention de l’insuffisance cardiaque, s’imposent.
© 2021 The Authors.
Figures
References
-
- Lloyd-Jones D.M., Wang T.J., Leip E.P., et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–1046. - PubMed
-
- Miyasaka Y., Barnes M.E., Gersh B.J., et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Wolf P.A., Abbott R.D., Kannel W.B. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- Benjamin E.J., Wolf P.A., D’Agostino R.B., et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–952. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
