

A Simple Subjective Evaluation of Enface OCT Reflectance Images Distinguishes Glaucoma From Healthy Eyes
- PMID: 34036303
- PMCID: PMC8161697
- DOI: 10.1167/tvst.10.6.31
A Simple Subjective Evaluation of Enface OCT Reflectance Images Distinguishes Glaucoma From Healthy Eyes
Abstract
Purpose: We present a subjective approach to detecting glaucomatous defects in enface images and assess its diagnostic performance. We also test the hypothesis that if reflectivity changes precede thickness changes in glaucoma there should be reduced correlation between the modalities in glaucoma compared to controls.
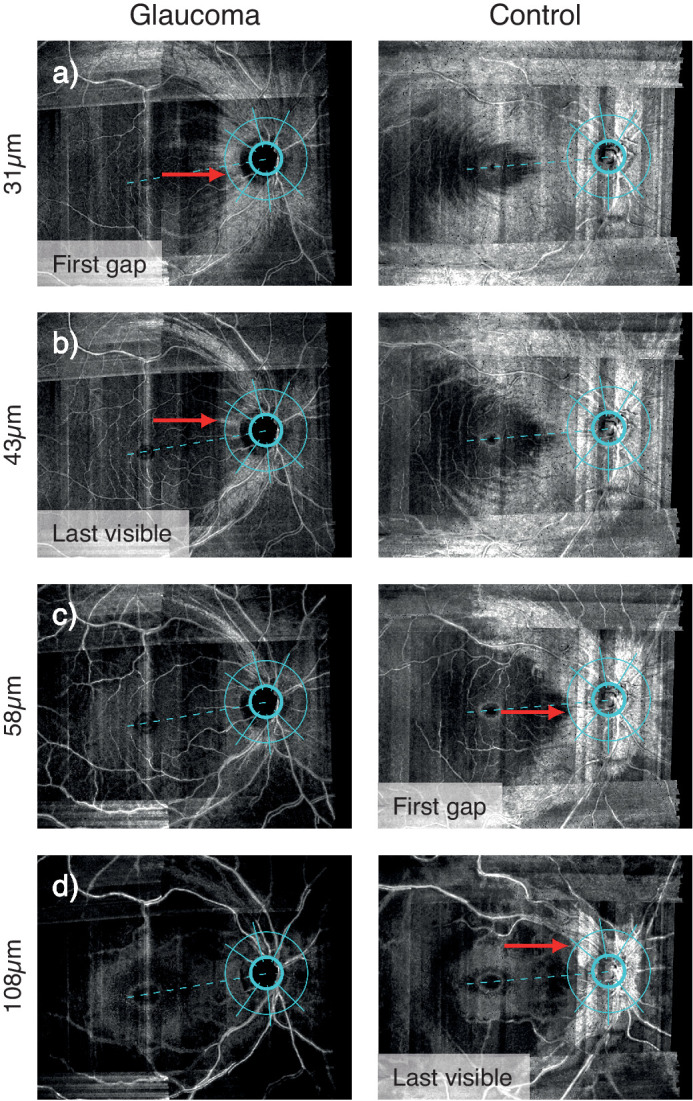
Methods: Twenty glaucoma participants and 20 age-matched controls underwent high-resolution OCT scans of one eye. 4 µm-thick enface slabs were constructed through the retina. Enface indices were depths of first gap in visible retinal nerve fiber bundles (RNFBs) and last visible bundle, subjectively evaluated in six sectors of a 3.5 mm circle around the optic disc. Retinal nerve fiber layer thickness (RNFLT) along the same circle was extracted at angles corresponding to enface indices. Between-group differences were tested by linear mixed models. Diagnostic performance was measured by partial receiver operating characteristic area (pAUC).
Results: First gap and last visible bundle were closer to the inner limiting membrane in glaucoma eyes (both P < 0.0001). Enface indices showed excellent diagnostic performance (pAUCs 0.63-1.00), similar to RNFLT (pAUCs 0.63-0.95). Correlation between enface and RNFLT parameters was strong in healthy (r = 0.81-0.92) and glaucoma eyes (r = 0.73-0.80).
Conclusions: This simple subjective method reliably identifies glaucomatous defects in enface images with diagnostic performance at least as good as existing thickness indices. Thickness and reflectivity were similarly related in healthy and glaucoma eyes, providing no strong evidence of reflectivity loss preceding thinning. Objective analyses may realize further potential of enface OCT images in glaucoma.
Translational relevance: Novel enface OCT indices may aid glaucoma diagnosis.
Conflict of interest statement
Disclosure:
Figures





References
-
- Prum BE Jr., Rosenberg LF, Gedde SJ, et al.. Primary open-angle glaucoma preferred practice pattern guidelines. Ophthalmology. 2016; 123(1): p41–p111. - PubMed
-
- National Institute of Health and Care Excellence. Glaucoma: diagnosis and management 2017 [Available from: https://www.nice.org.uk/guidance/ng81]. - PubMed
-
- Fallon M, Valero O, Pazos M, Anton A. Diagnostic accuracy of imaging devices in glaucoma: a meta-analysis. Surv Ophthalmol. 2017; 62(4): 446–461. - PubMed
-
- Tatham AJ, Medeiros FA, Zangwill LM, Weinreb RN.. Strategies to improve early diagnosis in glaucoma. Prog Brain Res. 2015; 221: 103–133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
