

Current Ceftriaxone Dose Recommendations are Adequate for Most Critically Ill Children: Results of a Population Pharmacokinetic Modeling and Simulation Study
- PMID: 34036552
- PMCID: PMC8505376
- DOI: 10.1007/s40262-021-01035-9
Current Ceftriaxone Dose Recommendations are Adequate for Most Critically Ill Children: Results of a Population Pharmacokinetic Modeling and Simulation Study
Abstract
Background and objective: Ceftriaxone is a cornerstone antibiotic for critically ill children with severe infections. Despite its widespread use, information on the pharmacokinetics of ceftriaxone is lacking in this population. We aimed to determine ceftriaxone pharmacokinetics in critically ill children and to propose ceftriaxone dosing guidelines resulting in adequate target attainment using population pharmacokinetic modeling and simulation.
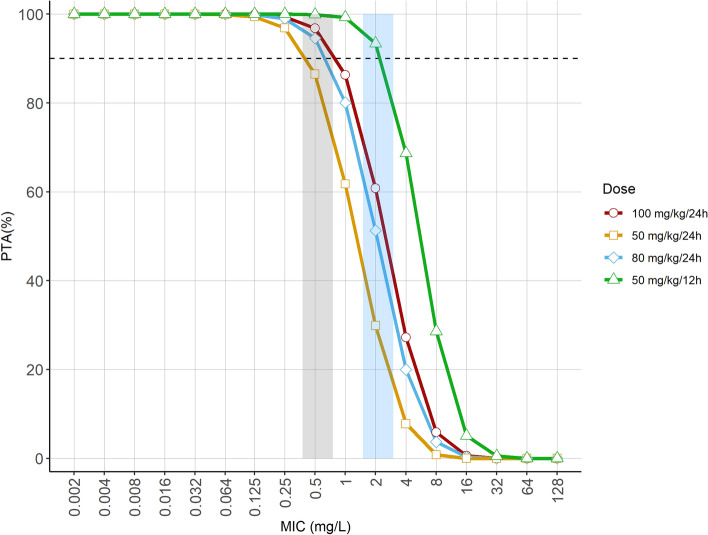
Methods: Critically ill children (aged 0-18 years) treated with intravenous ceftriaxone (100 mg/kg once daily, infused in 30 minutes) and a central or arterial line in place were eligible. Opportunistic blood sampling for total and unbound ceftriaxone concentrations was used. Population pharmacokinetic analysis was performed using non-linear mixed-effects modeling on NONMEM™ Version 7.4.3. Simulations were performed to select optimal doses using probability of target attainment for two pharmacokinetic targets of the minimum inhibitory concentration (MIC) reflecting the susceptibility of pathogens (f T > MIC 100% and fT > 4 × MIC 100%).
Results: Two hundred and five samples for total and 43 time-matched samples for unbound plasma ceftriaxone concentrations were collected from 45 patients, median age 2.5 (range 0.1-16.7) years. A two-compartment model with bodyweight as the co-variate for volume of distribution and clearance, and creatinine-based estimated glomerular filtration rate as an additional covariate for clearance, best described ceftriaxone pharmacokinetics. For a typical patient (2.5 years, 14 kg) with an estimated glomerular filtration rate of 80 mL/min/1.73 m2, the current 100-mg/kg once-daily dose results in a probability of target attainment of 96.8% and 60.8% for a MIC of 0.5 mg/L and 4 × MIC (2 mg/L), respectively, when using fT > MIC 100% as a target. For a 50-mg/kg twice-daily regimen, the probability of target attainment was 99.9% and 93.4%, respectively.
Conclusions: The current dosing regimen of ceftriaxone provides adequate exposure for susceptible pathogens in most critically ill children. In patients with an estimated glomerular filtration rate of > 80 mL/min/1.73 m2 or in areas with a high prevalence of less-susceptible pathogens (MIC ≥ 0.5 mg/L), a twice-daily dosing regimen of 50 mg/kg can be considered to improve target attainment.
Clinical trial registration: POPSICLE study (ClinicalTrials.gov, NCT03248349, registered 14 August, 2017), PERFORM study (ClinicalTrials.gov, NCT03502993, registered 19 April, 2018).
© 2021. The Author(s).
Conflict of interest statement
Roger J. Brüggemann has no conflicts of interest that are directly relevant to the content of this article. Outside of this work, he has served as consultant to and has received unrestricted research grants from Astellas Pharma Inc., F2G, Amplyx, Gilead Sciences, Merck Sharpe and Dohme Corp., and Pfizer Inc. All payments were invoiced by the Radboud University Medical Centre. Saskia N. de Wildt has no conflicts of interest that are directly relevant to the content of this article. Outside of this work she has served as consultant to and had received unrestricted research grant or in kind support from UCB Pharma, Spingotec, and Pfizer Inc. Saskia N. de Wildt is the director of the Dutch Pediatric Formulary and its internationally licensed versions (Stichting Nederlands Kenniscentrum Pharmacotherapy voor Kinderen & Kinderformularium B.V.) All payments were invoiced by the Radboud University Medical Centre. Stan J.F. Hartman, Parth J. Upadhyay, Nienke N. Hagedoorn, Ron A.A. Mathôt, Henriëtte A. Moll, Michiel van der Flier, Michiel F. Schreuder, and Catherijne A. Knibbe have no conflicts of interest that are directly relevant to the content of this article.
Figures


Similar articles
-
Population pharmacokinetic modeling of ceftriaxone in cerebrospinal fluid in children: should we be using once- or twice-daily dosing for meningitis?Antimicrob Agents Chemother. 2024 Nov 6;68(11):e0074724. doi: 10.1128/aac.00747-24. Epub 2024 Oct 8. Antimicrob Agents Chemother. 2024. PMID: 39377581 Free PMC article.
-
Role of renal function in risk assessment of target non-attainment after standard dosing of meropenem in critically ill patients: a prospective observational study.Crit Care. 2017 Oct 21;21(1):263. doi: 10.1186/s13054-017-1829-4. Crit Care. 2017. PMID: 29058601 Free PMC article.
-
Identifying optimal dosing strategies for meropenem in the paediatric intensive care unit through modelling and simulation.J Antimicrob Chemother. 2024 Oct 1;79(10):2668-2677. doi: 10.1093/jac/dkae274. J Antimicrob Chemother. 2024. PMID: 39092928 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Corticosteroids for the treatment of Duchenne muscular dystrophy.Cochrane Database Syst Rev. 2016 May 5;2016(5):CD003725. doi: 10.1002/14651858.CD003725.pub4. Cochrane Database Syst Rev. 2016. PMID: 27149418 Free PMC article.
Cited by
-
Pharmacokinetics of Antibiotics in Pediatric Intensive Care: Fostering Variability to Attain Precision Medicine.Antibiotics (Basel). 2021 Sep 28;10(10):1182. doi: 10.3390/antibiotics10101182. Antibiotics (Basel). 2021. PMID: 34680763 Free PMC article. Review.
-
Unraveling Ceftriaxone Dosing: Free Drug Prediction, Threshold Optimization, and Model Validation.AAPS J. 2025 Feb 26;27(2):50. doi: 10.1208/s12248-025-01041-w. AAPS J. 2025. PMID: 40011393
-
Getting the dose right using physiologically-based pharmacokinetic modeling: dexamethasone to prevent post-extubation stridor in children as proof of concept.Front Pediatr. 2024 Jul 5;12:1416440. doi: 10.3389/fped.2024.1416440. eCollection 2024. Front Pediatr. 2024. PMID: 39035463 Free PMC article.
-
Population Pharmacokinetic Modeling of Total and Free Ceftriaxone in Critically Ill Children and Young Adults and Monte Carlo Simulations Support Twice Daily Dosing for Target Attainment.Antimicrob Agents Chemother. 2022 Jan 18;66(1):e0142721. doi: 10.1128/AAC.01427-21. Epub 2021 Oct 11. Antimicrob Agents Chemother. 2022. PMID: 34633847 Free PMC article.
-
An Overview of the Protein Binding of Cephalosporins in Human Body Fluids: A Systematic Review.Front Pharmacol. 2022 Jun 28;13:900551. doi: 10.3389/fphar.2022.900551. eCollection 2022. Front Pharmacol. 2022. PMID: 35837288 Free PMC article.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
