

Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review
- PMID: 34037731
- PMCID: PMC8155823
- DOI: 10.1001/jamanetworkopen.2021.11417
Assessment of the Frequency and Variety of Persistent Symptoms Among Patients With COVID-19: A Systematic Review
Abstract
Importance: Infection with COVID-19 has been associated with long-term symptoms, but the frequency, variety, and severity of these complications are not well understood. Many published commentaries have proposed plans for pandemic control that are primarily based on mortality rates among older individuals without considering long-term morbidity among individuals of all ages. Reliable estimates of such morbidity are important for patient care, prognosis, and development of public health policy.
Objective: To conduct a systematic review of studies examining the frequency and variety of persistent symptoms after COVID-19 infection.
Evidence review: A search of PubMed and Web of Science was conducted to identify studies published from January 1, 2020, to March 11, 2021, that examined persistent symptoms after COVID-19 infection. Persistent symptoms were defined as those persisting for at least 60 days after diagnosis, symptom onset, or hospitalization or at least 30 days after recovery from the acute illness or hospital discharge. Search terms included COVID-19, SARS-CoV-2, coronavirus, 2019-nCoV, long-term, after recovery, long-haul, persistent, outcome, symptom, follow-up, and longitudinal. All English-language articles that presented primary data from cohort studies that reported the prevalence of persistent symptoms among individuals with SARS-CoV-2 infection and that had clearly defined and sufficient follow-up were included. Case reports, case series, and studies that described symptoms only at the time of infection and/or hospitalization were excluded. A structured framework was applied to appraise study quality.
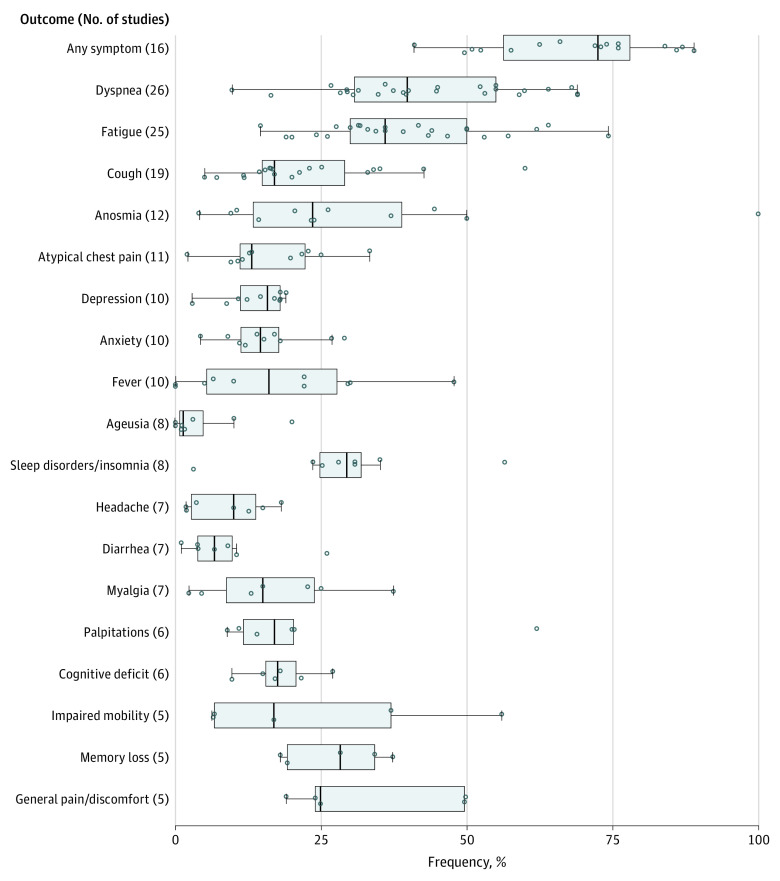
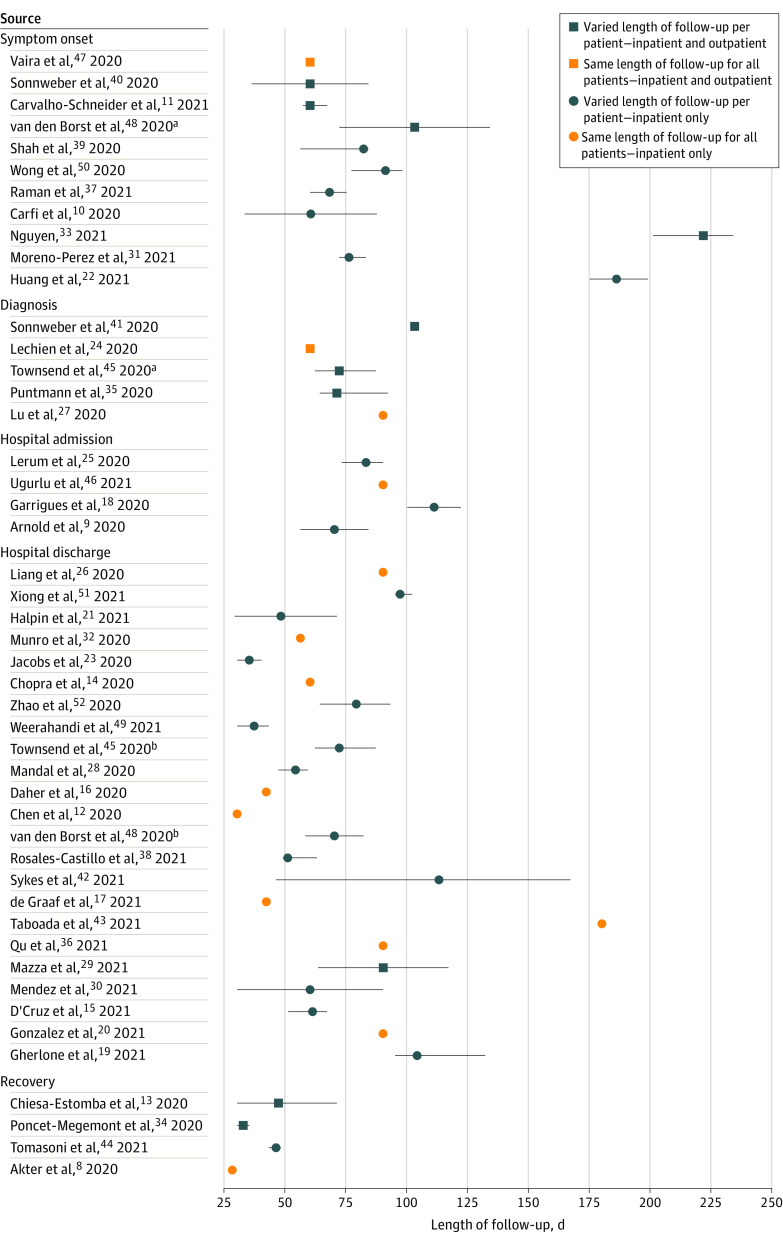
Findings: A total of 1974 records were identified; of those, 1247 article titles and abstracts were screened. After removal of duplicates and exclusions, 92 full-text articles were assessed for eligibility; 47 studies were deemed eligible, and 45 studies reporting 84 clinical signs or symptoms were included in the systematic review. Of 9751 total participants, 5266 (54.0%) were male; 30 of 45 studies reported mean or median ages younger than 60 years. Among 16 studies, most of which comprised participants who were previously hospitalized, the median proportion of individuals experiencing at least 1 persistent symptom was 72.5% (interquartile range [IQR], 55.0%-80.0%). Individual symptoms occurring most frequently included shortness of breath or dyspnea (26 studies; median frequency, 36.0%; IQR, 27.6%-50.0%), fatigue or exhaustion (25 studies; median frequency, 40.0%; IQR, 31.0%-57.0%), and sleep disorders or insomnia (8 studies; median 29.4%, IQR, 24.4%-33.0%). There were wide variations in the design and quality of the studies, which had implications for interpretation and often limited direct comparability and combinability. Major design differences included patient populations, definitions of time zero (ie, the beginning of the follow-up interval), follow-up lengths, and outcome definitions, including definitions of illness severity.
Conclusions and relevance: This systematic review found that COVID-19 symptoms commonly persisted beyond the acute phase of infection, with implications for health-associated functioning and quality of life. Current studies of symptom persistence are highly heterogeneous, and future studies need longer follow-up, improved quality, and more standardized designs to reliably quantify risks.
Conflict of interest statement
Figures
References
-
- Ahmed H, Patel K, Greenwood DC, et al. . Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: a systematic review and meta-analysis. J Rehabil Med. 2020;52(5):jrm00063. doi:10.2340/16501977-2694 - DOI - PubMed
-
- Mayo Clinic Staff. COVID-19 (coronavirus): long-term effects. Mayo Clinic. Updated April 8, 2021. Accessed October 20, 2020. https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coro...
-
- Centers for Disease Control and Prevention . Post-COVID conditions. Centers for Disease Control and Prevention. February 11, 2020. Updated April 8, 2021. Accessed October 20, 2020. https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects.html
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
