

Susceptibility-diffusion mismatch correlated with leptomeningeal collateralization in large vessel occlusion stroke
- PMID: 34038211
- PMCID: PMC8161861
- DOI: 10.1177/03000605211013179
Susceptibility-diffusion mismatch correlated with leptomeningeal collateralization in large vessel occlusion stroke
Abstract
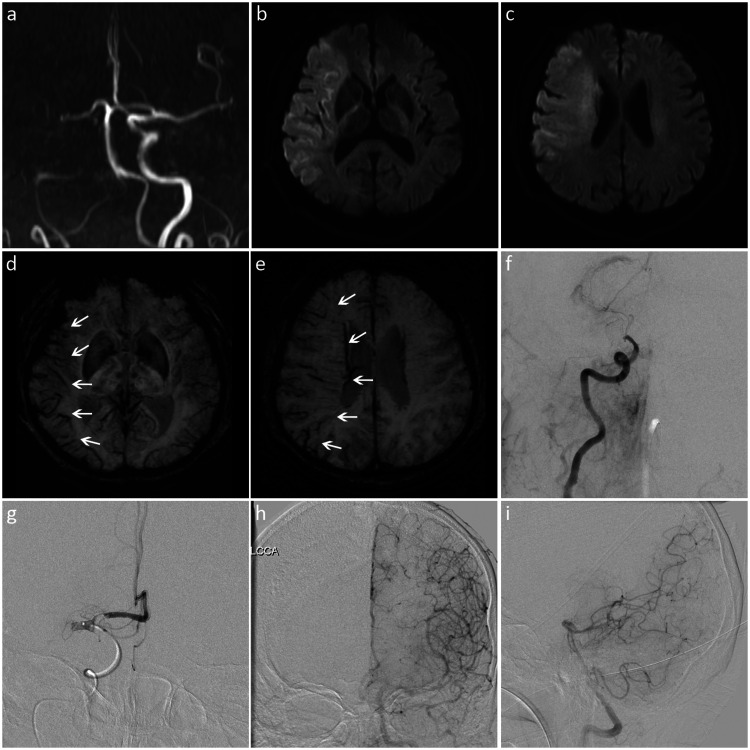
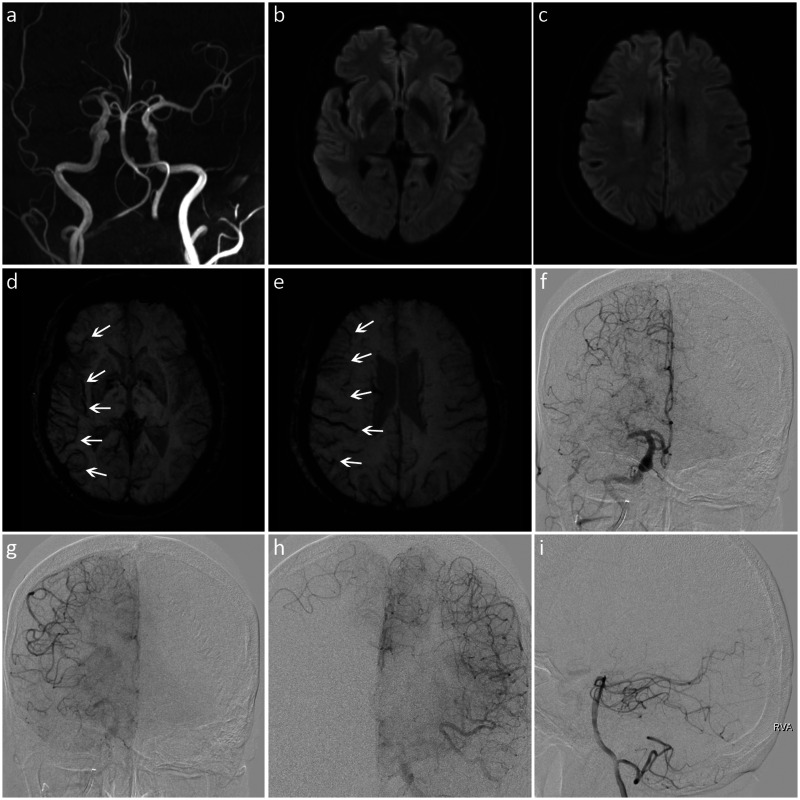
Objective: To investigate the relationship between asymmetric prominent hypointense vessels (prominent vessel sign, PVS) on susceptibility-weighted imaging (SWI) and leptomeningeal collateralization in patients with acute ischemic stroke due to large vessel occlusion.
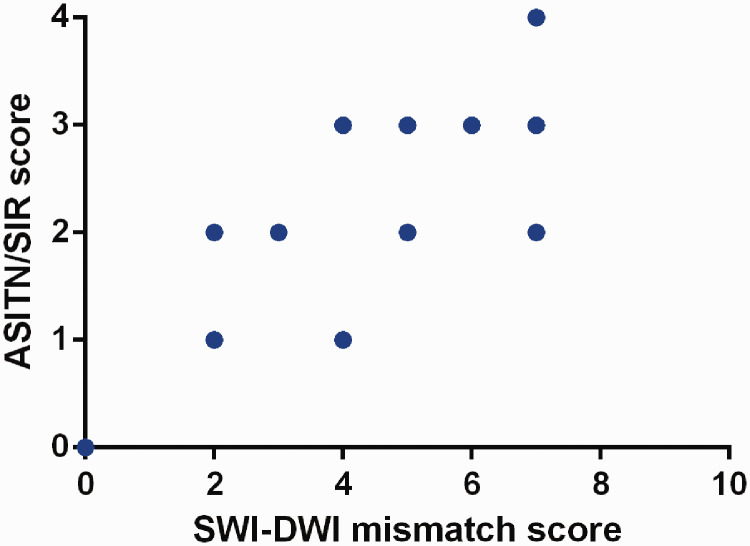
Methods: We retrospectively enrolled patients with M1 segment occlusion of the middle cerebral artery who underwent emergency magnetic resonance imaging and digital subtraction angiography within 24 hours from stroke onset. The extent of PVS on SWI was assessed using the Alberta Stroke Program Early CT Score (ASPECTS). Leptomeningeal collateralization on digital subtraction angiography images was assessed using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) scale. Spearman's rank correlation test was performed to explore the correlation of ASITN/SIR scores with SWI-ASPECTS and SWI-diffusion-weighted imaging (DWI) mismatch scores.
Results: Thirty-five patients were enrolled. There was no significant correlation between SWI-ASPECTS and ASITN/SIR scores. However, SWI-DWI mismatch scores were positively correlated with ASITN/SIR scores.
Conclusion: The range of PVS on SWI did not closely reflect the collateral status, while the range of SWI-DWI mismatch was significantly correlated with the leptomeningeal collateralization. In patients with acute anterior circulation stroke due to large vessel occlusion, larger SWI-DWI mismatch was associated with better leptomeningeal collaterals.
Keywords: Acute ischemic stroke; diffusion-weighted imaging; large vessel occlusion; leptomeningeal collateralization; prominent vessel sign; susceptibility-weighted imaging.
Conflict of interest statement
Figures
References
-
- Liebeskind DS. Collateral circulation. Stroke 2003; 34: 2279–2284. - PubMed
-
- Ginsberg MD. The cerebral collateral circulation: relevance to pathophysiology and treatment of stroke. Neuropharmacology 2018; 134: 280–292. - PubMed
-
- Haacke EM, Xu Y, Cheng YC, et al.. Susceptibility weighted imaging (SWI). Magn Reson Med 2004; 52: 612–618. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
