

Immediate "Kangaroo Mother Care" and Survival of Infants with Low Birth Weight
- PMID: 34038632
- PMCID: PMC8108485
- DOI: 10.1056/NEJMoa2026486
Immediate "Kangaroo Mother Care" and Survival of Infants with Low Birth Weight
Abstract
Background: "Kangaroo mother care," a type of newborn care involving skin-to-skin contact with the mother or other caregiver, reduces mortality in infants with low birth weight (<2.0 kg) when initiated after stabilization, but the majority of deaths occur before stabilization. The safety and efficacy of kangaroo mother care initiated soon after birth among infants with low birth weight are uncertain.
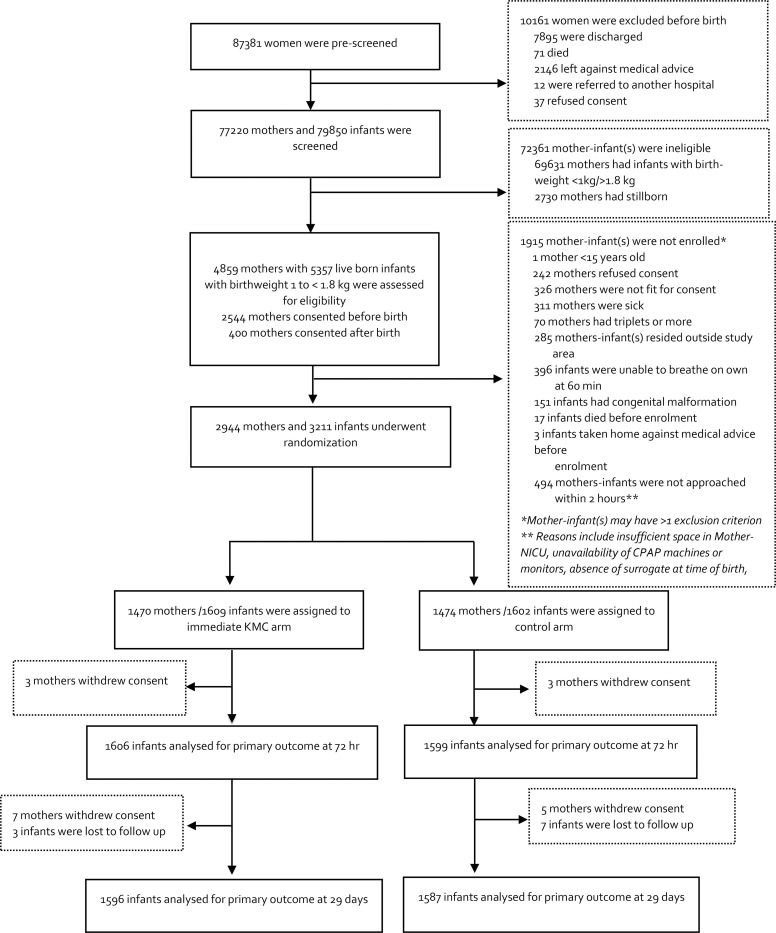
Methods: We conducted a randomized, controlled trial in five hospitals in Ghana, India, Malawi, Nigeria, and Tanzania involving infants with a birth weight between 1.0 and 1.799 kg who were assigned to receive immediate kangaroo mother care (intervention) or conventional care in an incubator or a radiant warmer until their condition stabilized and kangaroo mother care thereafter (control). The primary outcomes were death in the neonatal period (the first 28 days of life) and in the first 72 hours of life.
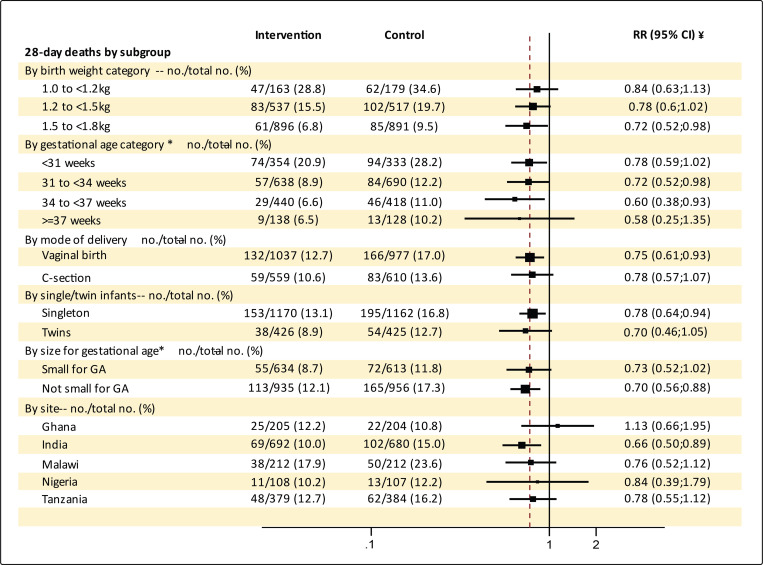
Results: A total of 3211 infants and their mothers were randomly assigned to the intervention group (1609 infants with their mothers) or the control group (1602 infants with their mothers). The median daily duration of skin-to-skin contact in the neonatal intensive care unit was 16.9 hours (interquartile range, 13.0 to 19.7) in the intervention group and 1.5 hours (interquartile range, 0.3 to 3.3) in the control group. Neonatal death occurred in the first 28 days in 191 infants in the intervention group (12.0%) and in 249 infants in the control group (15.7%) (relative risk of death, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P = 0.001); neonatal death in the first 72 hours of life occurred in 74 infants in the intervention group (4.6%) and in 92 infants in the control group (5.8%) (relative risk of death, 0.77; 95% CI, 0.58 to 1.04; P = 0.09). The trial was stopped early on the recommendation of the data and safety monitoring board owing to the finding of reduced mortality among infants receiving immediate kangaroo mother care.
Conclusions: Among infants with a birth weight between 1.0 and 1.799 kg, those who received immediate kangaroo mother care had lower mortality at 28 days than those who received conventional care with kangaroo mother care initiated after stabilization; the between-group difference favoring immediate kangaroo mother care at 72 hours was not significant. (Funded by the Bill and Melinda Gates Foundation; Australian New Zealand Clinical Trials Registry number, ACTRN12618001880235; Clinical Trials Registry-India number, CTRI/2018/08/015369.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
Immediate 'Kangaroo Mother Care' and survival of infants with low birth weight.Acta Paediatr. 2022 Feb;111(2):445-446. doi: 10.1111/apa.16117. Epub 2021 Oct 21. Acta Paediatr. 2022. PMID: 34674298 No abstract available.
References
-
- WHO/UNICEF. Low birthweight : country, regional and global estimates [Internet]. Available from: https://apps.who.int/iris/handle/10665/43184
-
- Lawn JE, Cousens S, Zupan J, Lancet Neonatal Survival Steering Team. 4 Million neonatal deaths: When? Where? Why? Lancet. 2005;365(9462):891–900. - PubMed
-
- Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost?. Lancet 2014;384(9940):347–70. - PubMed
-
- WHO. Kangaroo Mother Care: a practical guide [Internet]. WHO. 2003. [cited 2020 Jul 7];Available from: http://www.who.int/maternal_child_adolescent/documents/9241590351/en/
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical