

Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial
- PMID: 34038699
- PMCID: PMC8491267
- DOI: 10.1164/rccm.202101-0030OC
Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial
Abstract
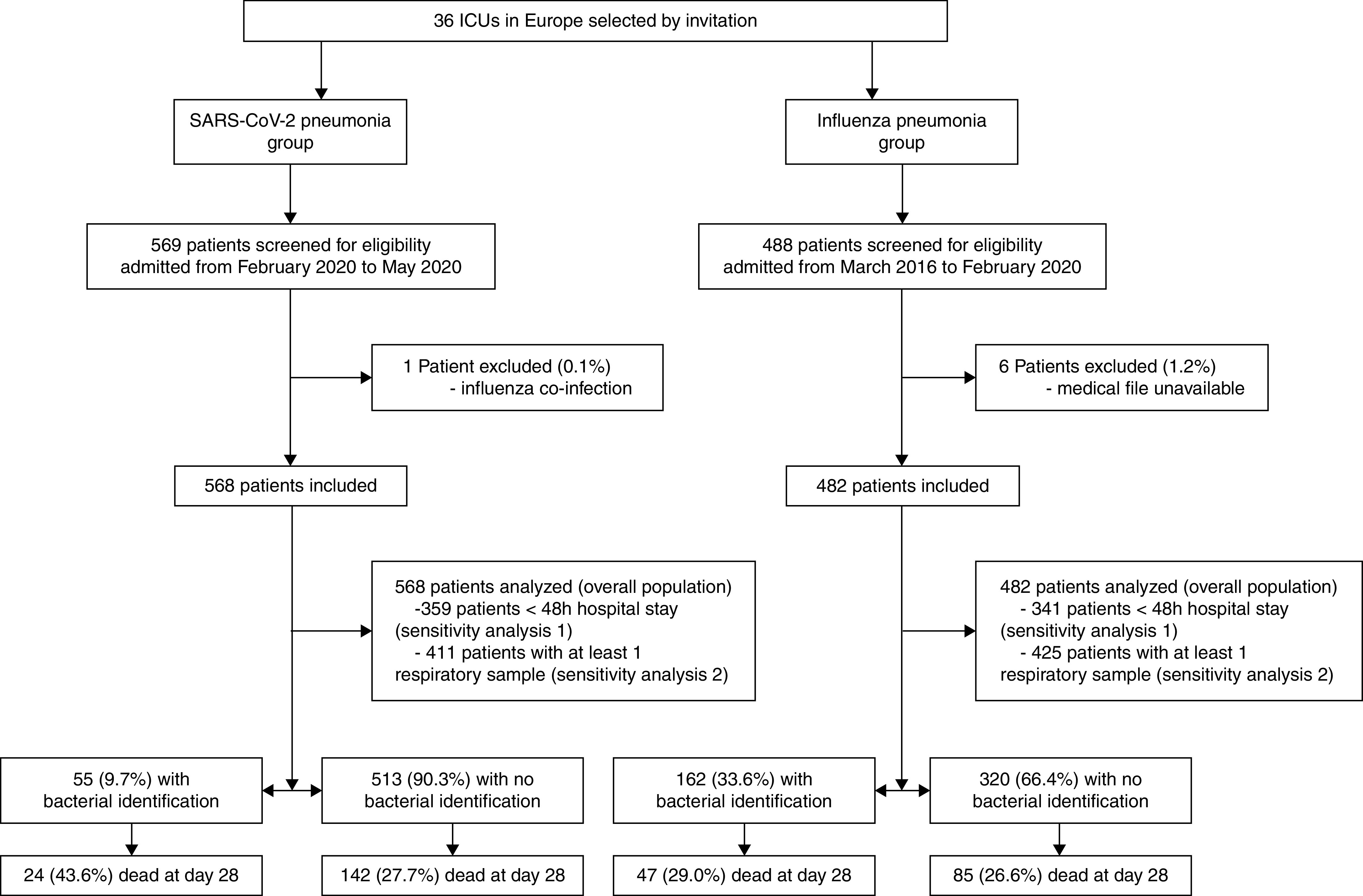
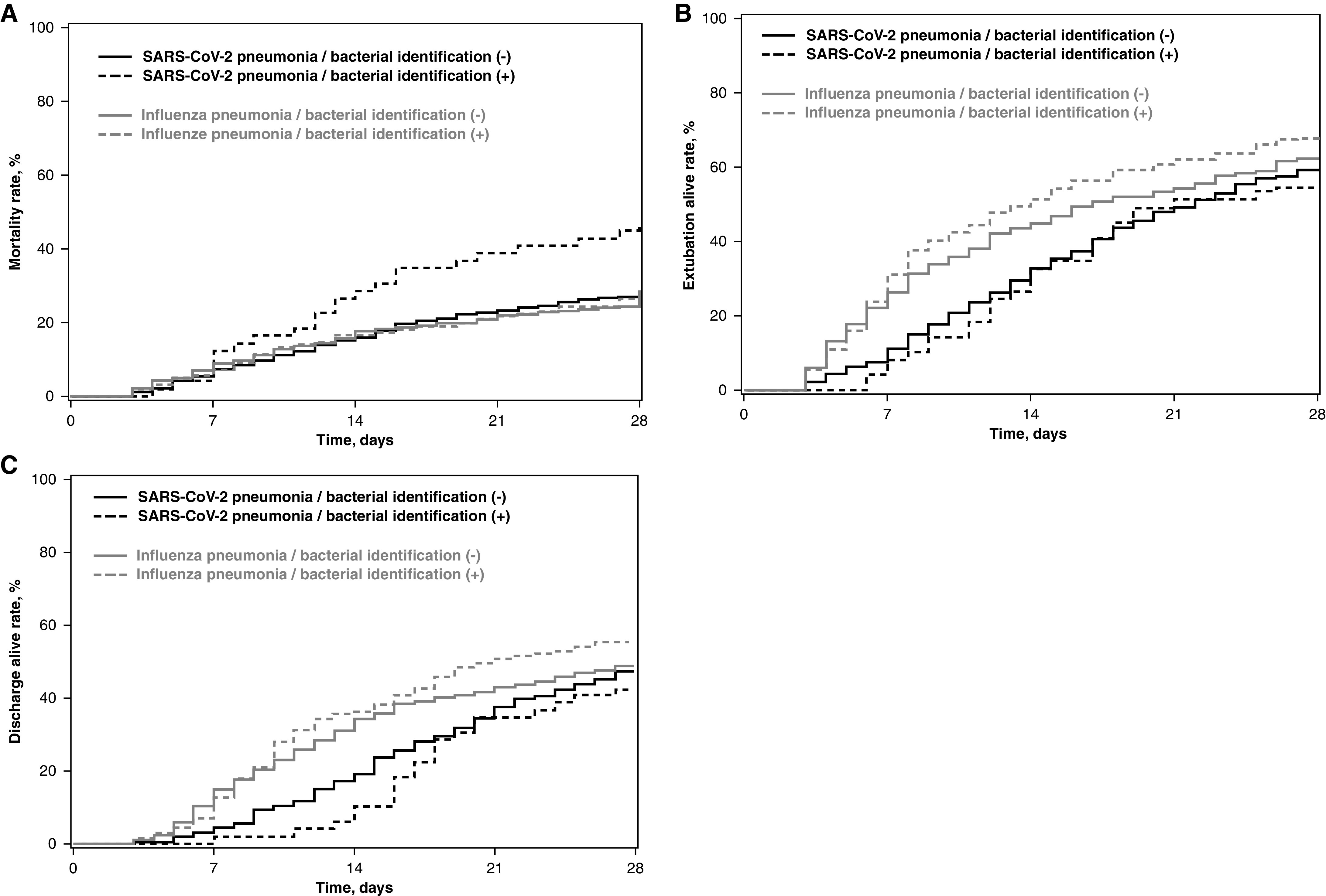
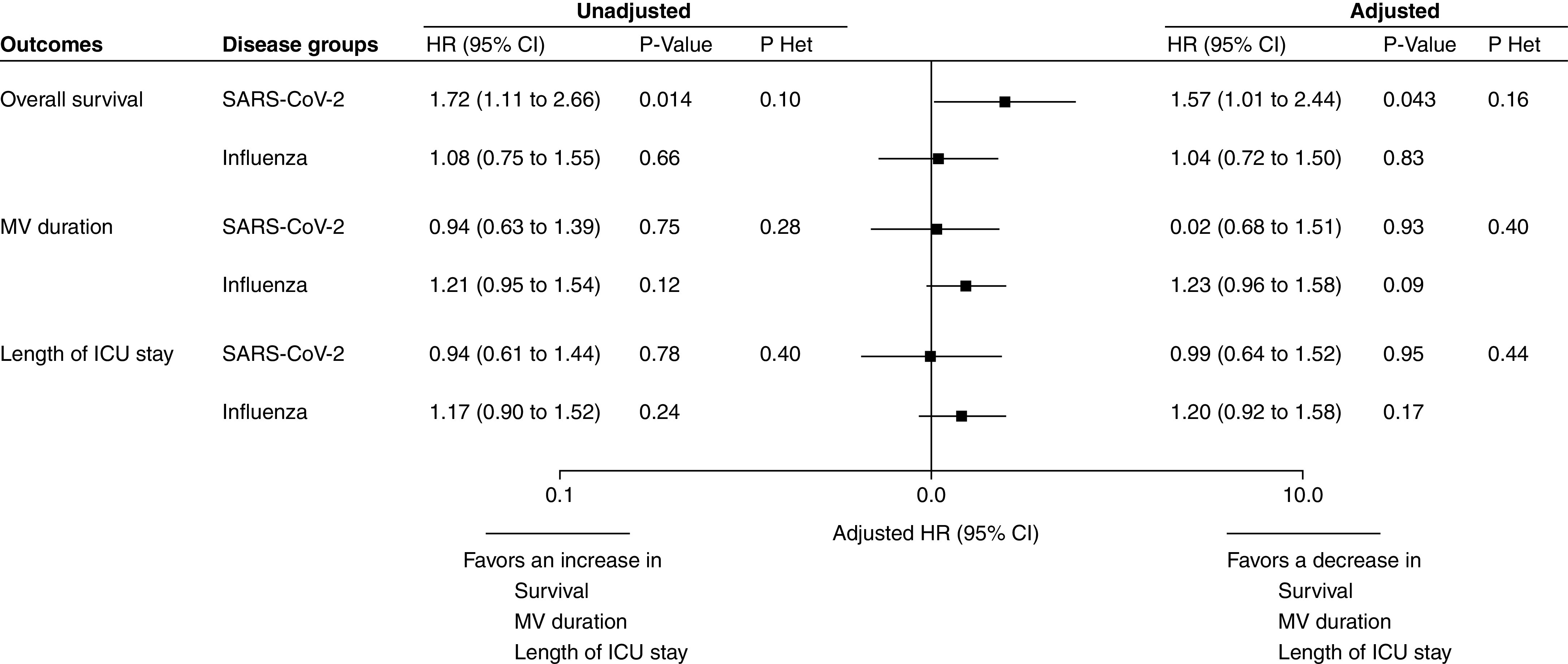
Rationale: Early empirical antimicrobial treatment is frequently prescribed to critically ill patients with coronavirus disease (COVID-19) based on Surviving Sepsis Campaign guidelines.Objectives: We aimed to determine the prevalence of early bacterial identification in intubated patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia, as compared with influenza pneumonia, and to characterize its microbiology and impact on outcomes.Methods: A multicenter retrospective European cohort was performed in 36 ICUs. All adult patients receiving invasive mechanical ventilation >48 hours were eligible if they had SARS-CoV-2 or influenza pneumonia at ICU admission. Bacterial identification was defined by a positive bacterial culture within 48 hours after intubation in endotracheal aspirates, BAL, blood cultures, or a positive pneumococcal or legionella urinary antigen test.Measurements and Main Results: A total of 1,050 patients were included (568 in SARS-CoV-2 and 482 in influenza groups). The prevalence of bacterial identification was significantly lower in patients with SARS-CoV-2 pneumonia compared with patients with influenza pneumonia (9.7 vs. 33.6%; unadjusted odds ratio, 0.21; 95% confidence interval [CI], 0.15-0.30; adjusted odds ratio, 0.23; 95% CI, 0.16-0.33; P < 0.0001). Gram-positive cocci were responsible for 58% and 72% of coinfection in patients with SARS-CoV-2 and influenza pneumonia, respectively. Bacterial identification was associated with increased adjusted hazard ratio for 28-day mortality in patients with SARS-CoV-2 pneumonia (1.57; 95% CI, 1.01-2.44; P = 0.043). However, no significant difference was found in the heterogeneity of outcomes related to bacterial identification between the two study groups, suggesting that the impact of coinfection on mortality was not different between patients with SARS-CoV-2 and influenza.Conclusions: Bacterial identification within 48 hours after intubation is significantly less frequent in patients with SARS-CoV-2 pneumonia than patients with influenza pneumonia.Clinical trial registered with www.clinicaltrials.gov (NCT04359693).
Keywords: SARS-CoV-2; bacterial; influenza; intensive care; mechanical ventilation.
Figures
Comment in
-
Bacterial Coinfection in COVID-19 and Influenza Pneumonia.Am J Respir Crit Care Med. 2021 Sep 1;204(5):498-500. doi: 10.1164/rccm.202106-1467ED. Am J Respir Crit Care Med. 2021. PMID: 34233146 Free PMC article. No abstract available.
-
The Mystery of Futility of Appropriate Antibiotics for Coinfection in COVID-19.Am J Respir Crit Care Med. 2021 Dec 15;204(12):1489. doi: 10.1164/rccm.202107-1656LE. Am J Respir Crit Care Med. 2021. PMID: 34546862 Free PMC article. No abstract available.
References
-
- European Centre for Disease Prevention and Control. 2021. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
