

Nrg1β Released in Remote Ischemic Preconditioning Improves Myocardial Perfusion and Decreases Ischemia/Reperfusion Injury via ErbB2-Mediated Rescue of Endothelial Nitric Oxide Synthase and Abrogation of Trx2 Autophagy
- PMID: 34039018
- PMCID: PMC8288485
- DOI: 10.1161/ATVBAHA.121.315957
Nrg1β Released in Remote Ischemic Preconditioning Improves Myocardial Perfusion and Decreases Ischemia/Reperfusion Injury via ErbB2-Mediated Rescue of Endothelial Nitric Oxide Synthase and Abrogation of Trx2 Autophagy
Abstract
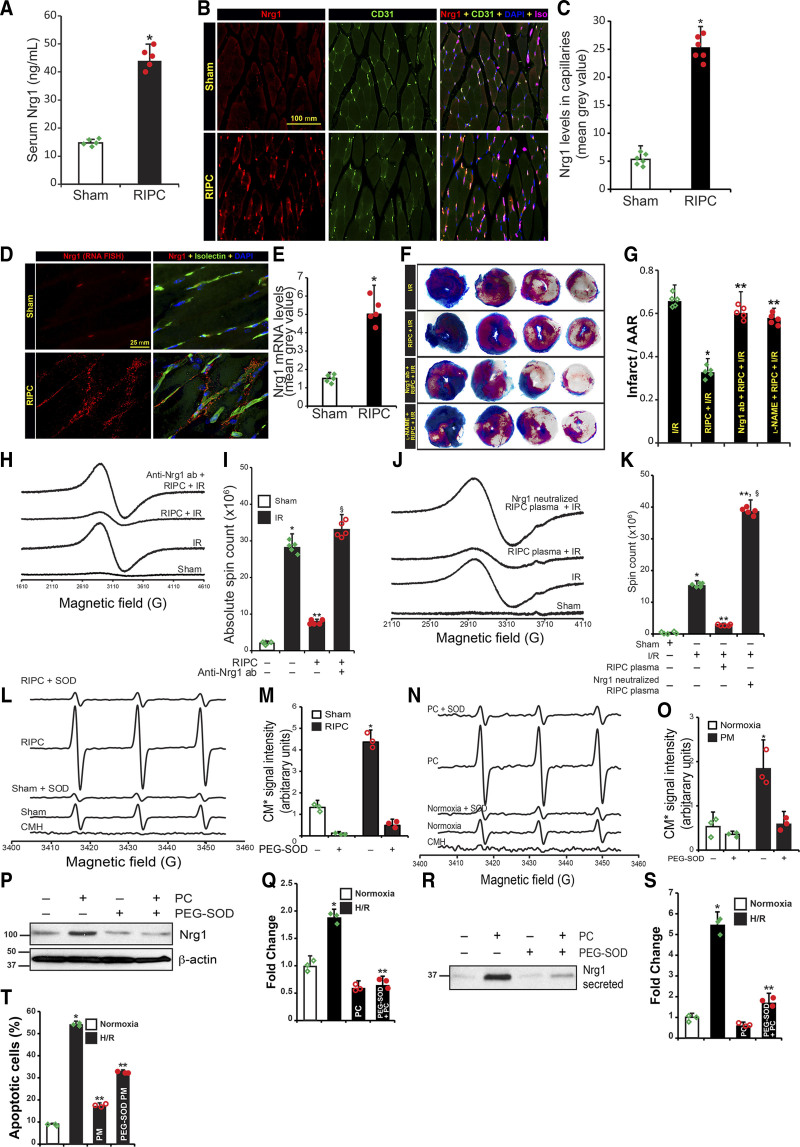
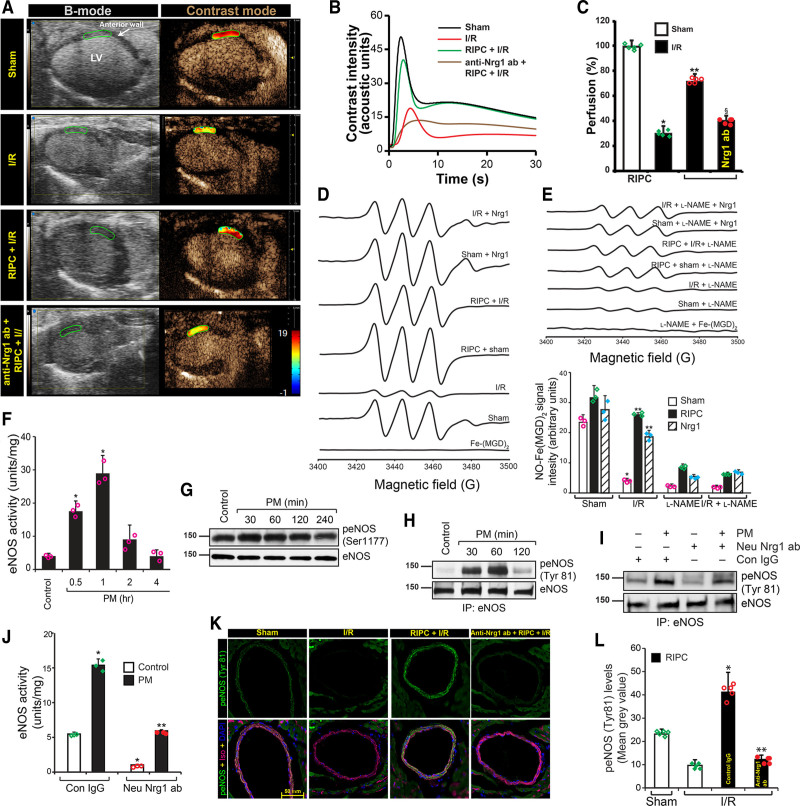
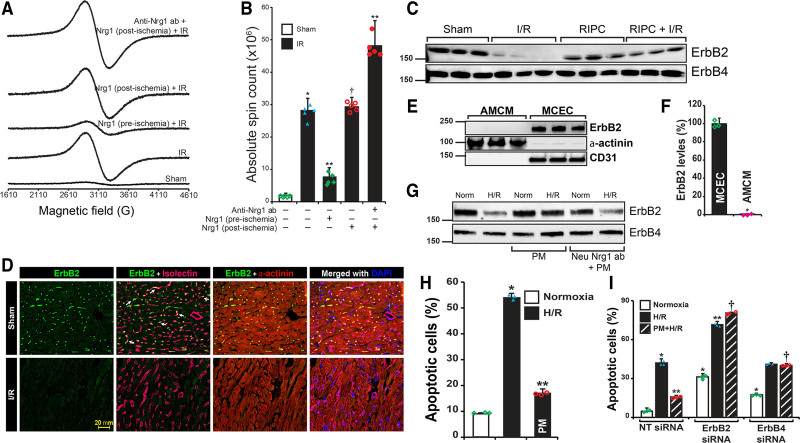
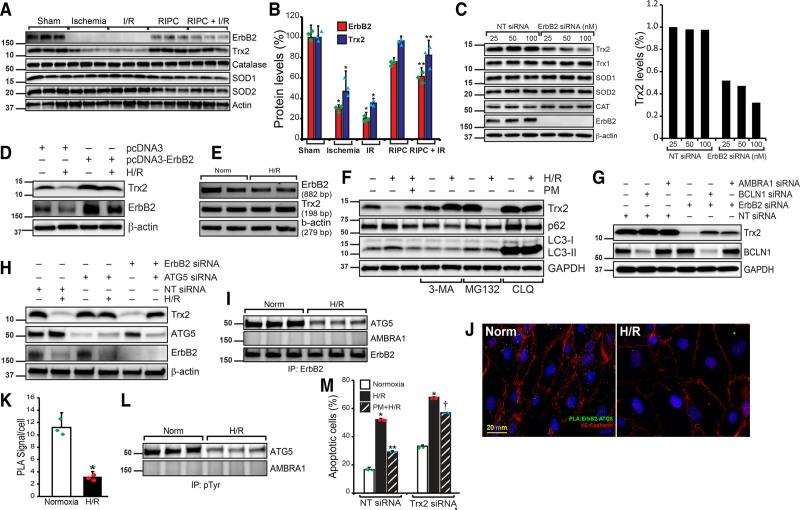
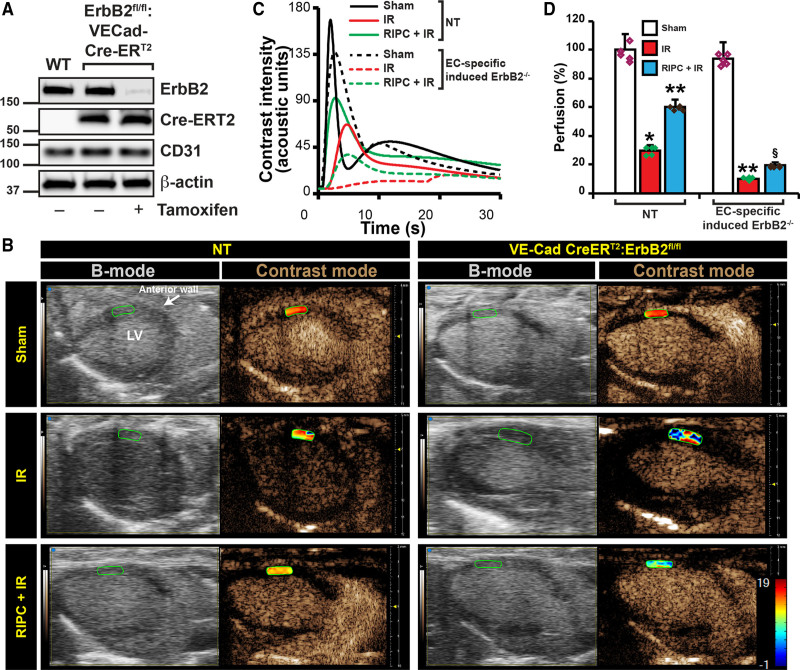
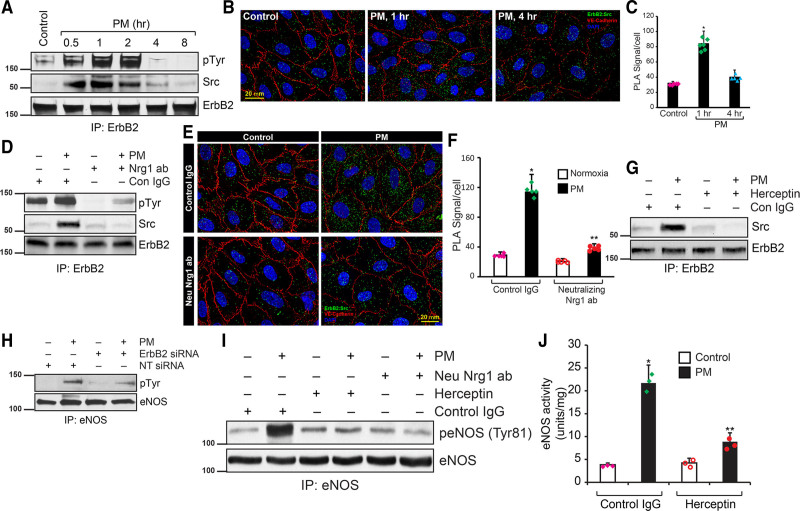
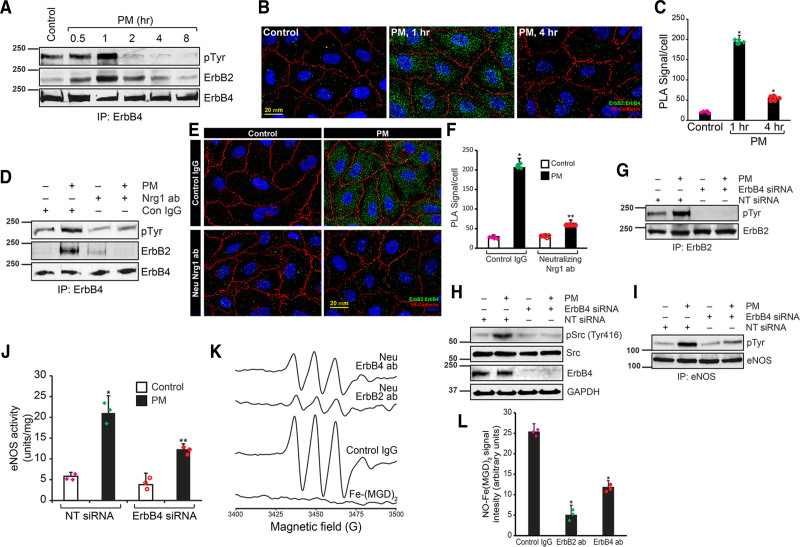
OBJECTIVE: Remote ischemic preconditioning (RIPC) is an intervention process where the application of multiple cycles of short ischemia/reperfusion (I/R) in a remote vascular bed provides protection against I/R injury. However, the identity of the specific RIPC factor and the mechanism by which RIPC alleviates I/R injury remains unclear. Here, we have investigated the identity and the mechanism by which the RIPC factor provides protection. APPROACH AND RESULTS: Using fluorescent in situ hybridization and immunofluorescence, we found that RIPC induces Nrg1β expression in the endothelial cells, which is secreted into the serum. Whereas, RIPC protected against myocardial apoptosis and infarction, treatment with neutralizing-Nrg1 antibodies abolished the protective effect of RIPC. Further, increased superoxide anion generated in RIPC is required for Nrg1 expression. Improved myocardial perfusion and nitric oxide production were achieved by RIPC as determined by contrast echocardiography and electron spin resonance. However, treatment with neutralizing-Nrg1β antibody abrogated these effects, suggesting Nrg1β is a RIPC factor. ErbB2 (Erb-B2 receptor tyrosine kinase 2) is not expressed in the adult murine cardiomyocytes, but expressed in the endothelial cells of heart which is degraded in I/R. RIPC-induced Nrg1β interacts with endothelial ErbB2 and thereby prevents its degradation. Mitochondrial Trx2 (thioredoxin) is degraded in I/R, but rescue of ErbB2 by Nrg1β prevents Trx-2 degradation that decreased myocardial apoptosis in I/R. CONCLUSIONS: Nrg1β is a RIPC factor that interacts with endothelial ErbB2 and prevents its degradation, which in turn prevents Trx2 degradation due to phosphorylation and inactivation of ATG5 (autophagy-related 5) by ErbB2. Nrg1β also restored loss of eNOS (endothelial nitric oxide synthase) function in I/R via its interaction with Src.
Figures
Comment in
-
Nrg1β as a Proangiogenesis Therapy: How Is Nrg1β Therapy Unique From Other Angiogenesis Therapies?Arterioscler Thromb Vasc Biol. 2021 Aug;41(8):2315-2317. doi: 10.1161/ATVBAHA.121.316513. Epub 2021 Jun 24. Arterioscler Thromb Vasc Biol. 2021. PMID: 34162231 Free PMC article. No abstract available.
References
-
- Hausenloy DJ, Yellon DM. Ischaemic conditioning and reperfusion injury. Nat Rev Cardiol. 2016; 13:193–209. doi: 10.1038/nrcardio.2016.5 - PubMed
-
- Cung TT, Morel O, Cayla G, Rioufol G, Garcia-Dorado D, Angoulvant D, Bonnefoy-Cudraz E, Guérin P, Elbaz M, Delarche N, et al. . Cyclosporine before PCI in patients with acute myocardial infarction. N Engl J Med. 2015; 373:1021–1031. doi: 10.1056/NEJMoa1505489 - PubMed
-
- Heusch G. Molecular basis of cardioprotection: signal transduction in ischemic pre-, post-, and remote conditioning. Circ Res. 2015; 116:674–699. doi: 10.1161/CIRCRESAHA.116.305348 - PubMed
-
- Anttila V, Haapanen H, Yannopoulos F, Herajärvi J, Anttila T, Juvonen T. Review of remote ischemic preconditioning: from laboratory studies to clinical trials. Scand Cardiovasc J. 2016; 50:355–361. doi: 10.1080/14017431.2016.1233351 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
