

2D cine vs. 3D self-navigated free-breathing high-resolution whole heart cardiovascular magnetic resonance for aortic root measurements in congenital heart disease
- PMID: 34039356
- PMCID: PMC8157643
- DOI: 10.1186/s12968-021-00744-1
2D cine vs. 3D self-navigated free-breathing high-resolution whole heart cardiovascular magnetic resonance for aortic root measurements in congenital heart disease
Abstract
Background: Cardiovascular magnetic resonance (CMR) is considered the method of choice for evaluation of aortic root dilatation in congenital heart disease. Usually, a cross-sectional 2D cine stack is acquired perpendicular to the vessel's axis. However, this method requires a considerable patient collaboration and precise planning of image planes. The present study compares a recently introduced 3D self-navigated free-breathing high-resolution whole heart CMR sequence (3D self nav) allowing a multiplanar retrospective reconstruction of the aortic root as an alternative to the 2D cine technique for determination of aortic root diameters.
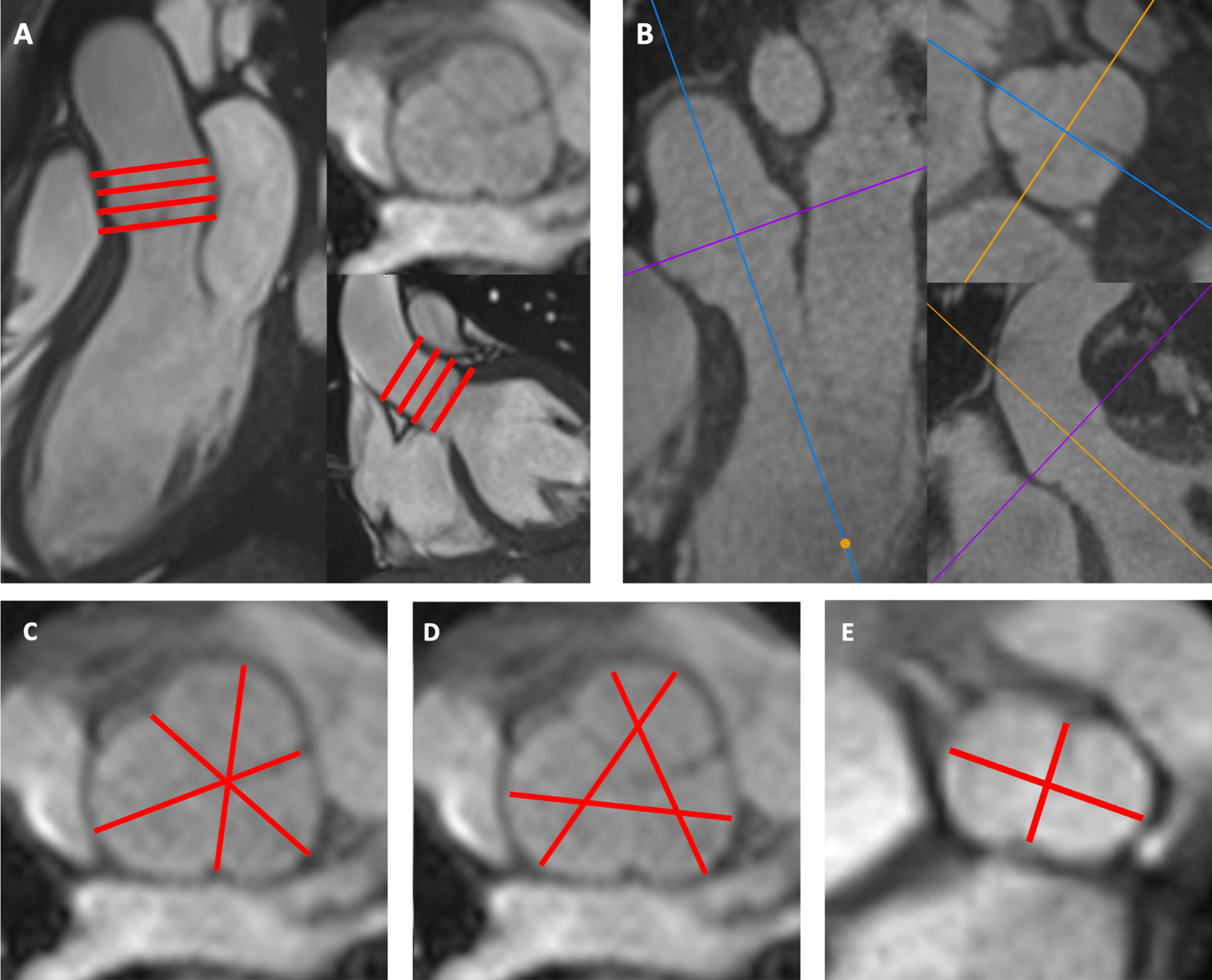
Methods: A total of 6 cusp-commissure (CuCo) and cusp-cusp (CuCu) enddiastolic diameters were measured by two observers on 2D cine and 3D self nav cross-sectional planes of the aortic root acquired on a 1.5 T CMR scanner. Asymmetry of the aortic root was evaluated by the ratio of the minimal to the maximum 3D self nav CuCu diameter. CuCu diameters were compared to standard transthoracic echocardiographic (TTE) aortic root diameters.
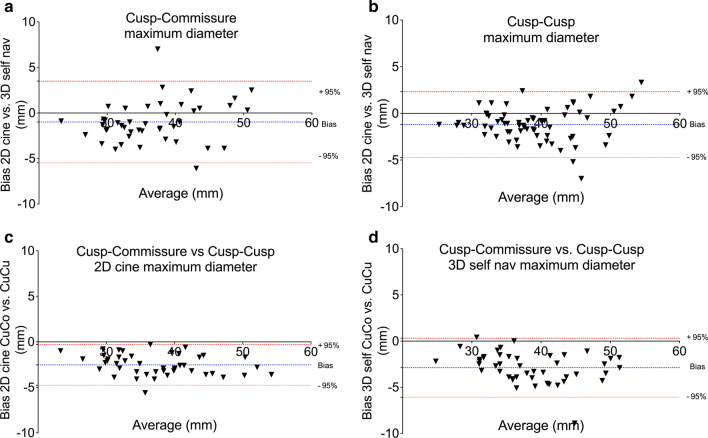
Results: Sixty-five exams in 58 patients (32 ± 15 years) were included. Typically, 2D cine and 3D self nav spatial resolution was 1.1-1.52 × 4.5-7 mm and 0.9-1.153 mm, respectively. 3D self nav yielded larger maximum diameters than 2D cine: CuCo 37.2 ± 6.4 vs. 36.2 ± 7.0 mm (p = 0.006), CuCu 39.7 ± 6.3 vs. 38.5 ± 6.5 mm (p < 0.001). CuCu diameters were significantly larger (2.3-3.9 mm, p < 0.001) than CuCo and TTE diameters on both 2D cine and 3D self nav. Intra- and interobserver variabilities were excellent for both techniques with bias of -0.5 to 1.0 mm. Intra-observer variability of the more experienced observer was better for 3D self nav (F-test p < 0.05). Aortic root asymmetry was more pronounced in patients with bicuspid aortic valve (BAV: 0.73 (interquartile (IQ) 0.69; 0.78) vs. 0.93 (IQ 0.9; 0.96), p < 0.001), which was associated to a larger difference of maximum CuCu to TTE diameters: 5.5 ± 3.3 vs. 3.3 ± 3.8 mm, p = 0.033.
Conclusion: Both, the 3D self nav and 2D cine CMR techniques allow reliable determination of aortic root diameters. However, we propose to privilege the 3D self nav technique and measurement of CuCu diameters to avoid underestimation of the maximum diameter, particularly in patients with asymmetric aortic roots and/or BAV.
Keywords: 3D self-navigation whole heart; Aortic root dilatation; Bicuspid aortic valve; Congenital heart disease.
Conflict of interest statement
CN, JB, TR, AP, MS and PM do not declare competing interest. DP is an employee of Siemens Healthcare and possesses stocks of Siemens Healthcare (conflict not relevant for this paper). JS receives annual funding of Bayer Healthcare, Switzerland. Dr. Tim Leiner served as a JCMR Guest Editor for this manuscript.
Figures
References
-
- Detaint D, Faivre L, Collod-Beroud G, Child AH, Loeys BL, Binquet C, Gautier E, Arbustini E, Mayer K, Arslan-Kirchner M, Stheneur C, Halliday D, Beroud C, Bonithon-Kopp C, Claustres M, Plauchu H, Robinson PN, Kiotsekoglou A, De Backer J, Ades L, Francke U, De Paepe A, Boileau C, Jondeau G. Cardiovascular manifestations in men and women carrying a FBN1 mutation. Eur Heart J. 2010;31:2223–2229. doi: 10.1093/eurheartj/ehq258. - DOI - PubMed
-
- Mortensen KH, Hjerrild BE, Stochholm K, Andersen NH, Sorensen KE, Lundorf E, Horlyck A, Pedersen EM, Christiansen JS, Gravholt CH. Dilation of the ascending aorta in Turner syndrome—a prospective cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2011;13:24. doi: 10.1186/1532-429X-13-24. - DOI - PMC - PubMed
-
- Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, Grabenwoger M, Haverich A, Iung B, Manolis AJ, Meijboom F, Nienaber CA, Roffi M, Rousseau H, Sechtem U, Sirnes PA, Allmen RS, Vrints CJ and Guidelines ESCCfP. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014;35:2873–926. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
