

Pathophysiology of decompensated cirrhosis: Portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction
- PMID: 34039492
- PMCID: PMC9272511
- DOI: 10.1016/j.jhep.2021.01.002
Pathophysiology of decompensated cirrhosis: Portal hypertension, circulatory dysfunction, inflammation, metabolism and mitochondrial dysfunction
Abstract
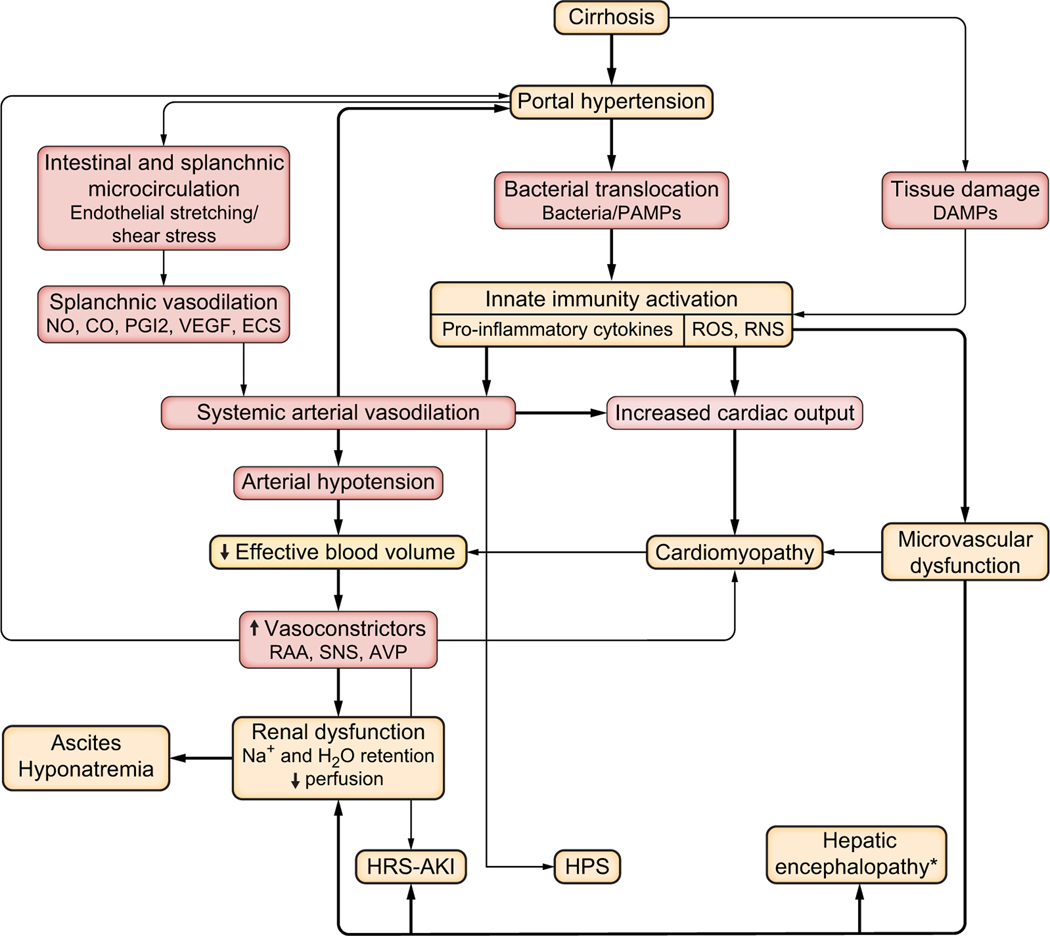
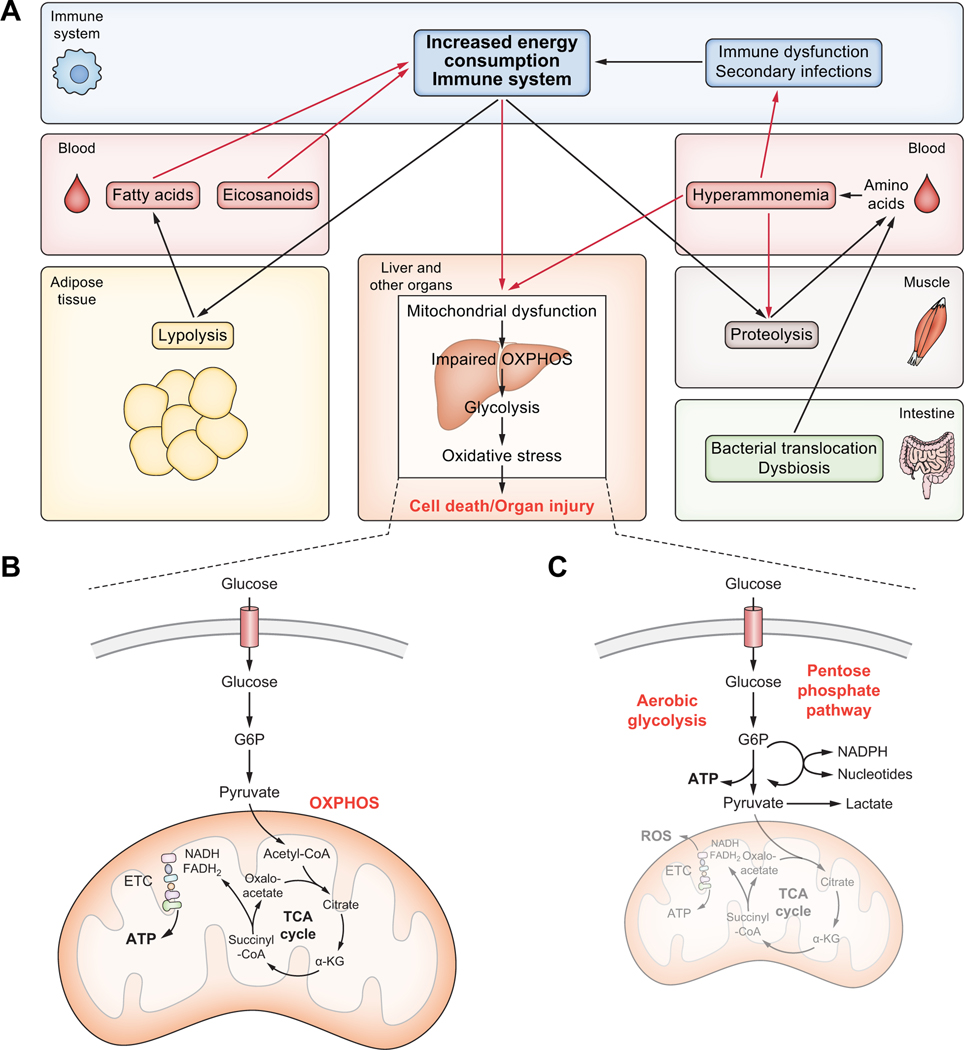
Patients with acutely decompensated cirrhosis have a dismal prognosis and frequently progress to acute-on-chronic liver failure, which is characterised by hepatic and extrahepatic organ failure(s). The pathomechanisms involved in decompensation and disease progression are still not well understood, and as specific disease-modifying treatments do not exist, research to identify novel therapeutic targets is of the utmost importance. This review amalgamates the latest knowledge on disease mechanisms that lead to tissue injury and extrahepatic organ failure - such as systemic inflammation, mitochondrial dysfunction, oxidative stress and metabolic changes - and marries these with the classical paradigms of acute decompensation to form a single paradigm. With this detailed breakdown of pathomechanisms, we identify areas for future research. Novel disease-modifying strategies that break the vicious cycle are urgently required to improve patient outcomes.
Keywords: ACLF; Acute-on-chronic liver failure; Ascites; Cirrhosis; DAMP; Hepatic encephalopathy; Organ failure; PAMP; Tissue injury; Variceal bleeding.
Copyright © 2021 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest Cornelius Engelmann has on-going research collaboration with Merz Pharmaceutical and Novartis. He has received speaker fees from Novartis, Gilead and Merz Pharmaceuticals. Jaime Bosch received consultancy fees from Actelion, Ambys, BioVie, BLB, BMS, Brudy, Chiasma, Exalenz, Gilead, Lipocine, Surrozen, Zydus and speaker fees from Gore. Mauro Bernardi received consultancy fees from CSL Behring GmbH, Grifols SA, Martin Pharmaceuticals and speaker fees from CSL Behring GmbH, Grifols SA, Takeda, PPTA, Octapharma AG. All other authors declared no conflict of interest. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures


References
-
- Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology 2013;144. 1426–1437, 1437 e1421–1429. - PubMed
-
- Arroyo V, Moreau R, Jalan R. Acute-on-Chronic liver failure. N Engl J Med 2020;382:2137–2145. - PubMed
-
- Gustot T, Fernandez J, Garcia E, Morando F, Caraceni P, Alessandria C, et al. Clinical Course of acute-on-chronic liver failure syndrome and effects on prognosis. Hepatology 2015;62:243–252. - PubMed
-
- Trebicka J, Fernandez J, Papp M, Caraceni P, Laleman W, Gambino C, et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J Hepatol 2020;73(4):842–854. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
